
Articles
- Page Path
- HOME > Headache Pain Res > Volume 26(2); 2025 > Article
-
Original Article
Clinical Characteristics of Migraine and Serum Beta-Endorphin Levels in Undergraduate Students in Osun State, Nigeria -
Adebimpe Ogunmodede1
 , Ahmed Idowu2, Ahmad Sanusi3, Uchenna Eke4, Akintunde Adebowale5, Michael Fawale6, Morenikeji Komolafe6
, Ahmed Idowu2, Ahmad Sanusi3, Uchenna Eke4, Akintunde Adebowale5, Michael Fawale6, Morenikeji Komolafe6 -
Headache and Pain Research 2025;26(2):162-170.
DOI: https://doi.org/10.62087/hpr.2025.0006
Published online: June 26, 2025
1Department of Medicine, Federal Medical Centre, Owo, Nigeria
2Stroke Department Royal Wolverhampton NHS Trust, Wolverhampton, United Kingdom
3Department of Medicine, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria
4Neurology Unit, Department of Medicine, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria
5Department of Neurology, Penn State Health Milton S. Hershey Medical Center, Hershey, PA, USA
6Department of Medicine, Obafemi Awolowo University, Ile-Ife, Nigeria
- Correspondence: Adebimpe Ogunmodede, MD Department of Medicine, Federal Medical Centre, Oba Road, Owo 341101, Ondo, Nigeria Tel: +234-8035094545, E-mail: bimpefunmilola@yahoo.com
© 2025 The Korean Headache Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,973 Views
- 31 Download
Abstract
-
Purpose
- Migraine is a common neurological disorder diagnosed using the International Classification of Headache Disorders (ICHD). Beta-endorphin has pain-reducing properties and may serve as a future prognostic marker for migraine. This study aimed to assess the clinical characteristics of migraine and compare serum beta-endorphin levels in migraine patients and healthy controls among young undergraduate students.
-
Methods
- This comparative cross-sectional study was conducted among undergraduate students at Obafemi Awolowo University, Nigeria. Fifty participants with migraine headaches were recruited using purposive sampling according to the ICHD-3 criteria. Healthy controls were recruited using convenience sampling and matched for age and sex. A study questionnaire was administered to all participants. Serum beta-endorphin concentrations in both migraineurs and healthy controls were measured using enzyme-linked immunosorbent assays. The beta-endorphin levels between migraine patients and healthy controls were compared using the Mann-Whitney U-test. The data were analyzed using SPSS version 26.0. A p-value of <0.05 was considered statistically significant.
-
Results
- A total of 12 males and 38 females were recruited in both groups. The most commonly used medication for acute migraine treatment was paracetamol, while amitriptyline was the most frequently used prophylactic. Median serum beta-endorphin levels were significantly lower in the migraine group, at 385.4 pg/mL (328.5–423.4 pg/mL), compared to the control group, at 442.9 pg/mL (357.5–477.6 pg/mL) (p=0.01).
-
Conclusion
- Serum beta-endorphin levels were significantly lower in young adults with migraine, suggesting a potential role for reduced endogenous analgesia in migraine pathophysiology. This supports the potential utility of beta-endorphin as a prognostic biomarker for migraine.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
AVAILABILITY OF DATA AND MATERIAL
The data presented in this study are available upon reasonable request from the corresponding author.
AUTHOR CONTRIBUTIONS
Conceptualization: AO, AI, AA; Data Curation: AS, UE; Supervision: MF, MK; Writing–original draft: AO, AI, AS, UE, AA; Writing–review & editing: AA, MF, MK. All authors read and approved the final manuscript.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING STATEMENT
Not applicable.
ACKNOWLEDGMENTS
We appreciate the staff of the Chemical Pathology Department of OAUTHC Ile-Ife for their assistance in the storage and analysis of the serum samples.



| Variable | Intervention group | Statistics | |
|---|---|---|---|
| Migraine headache group (n=50) | Healthy group (n=50) | ||
| Serum beta-endorphin (pg/mL) | 385.4 (328.5–423.4) | 442.9 (357.5–477.6) | U=843,000, p=0.01 |
| AUC | p-value | 95% CI | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Cut off value (pg/mL) | |
|---|---|---|---|---|---|---|---|---|
| Beta-endorphin | 0.70 | 0.01 | 0.54–0.77 | 64.0 | 71.4 | 66.7 | 69.6 | 403.4 |
- 1. Lin YK, Lin GY, Lee JT, et al. Associations between sleep quality and migraine frequency: a cross-sectional case-control study. Medicine (Baltimore) 2016;95:e3554.ArticlePubMedPMC
- 2. GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017;390:1211-1259.ArticlePubMedPMC
- 3. Ashina M. Migraine. N Engl J Med 2020;383:1866-1876.ArticlePubMed
- 4. Woldeamanuel YW, Andreou AP, Cowan RP. Prevalence of migraine headache and its weight on neurological burden in Africa: a 43-year systematic review and meta-analysis of community-based studies. J Neurol Sci 2014;342:1-15.ArticlePubMed
- 5. Aderinto N, Olatunji G, Kokori E, et al. Prevalence, characteristics, and treatment outcomes of migraine headache in Nigeria: a systematic review and meta-analysis. J Headache Pain 2024;25:172.ArticlePubMedPMCPDF
- 6. Mustapha AF, Fawale MB, Adebanjo OM, Arawomo A. A survey of headache among nursing students in a Nigerian university. Res J Health Sci 2023;7:39-47.
- 7. Sanya EO, Desalu OO, Aderibigbe SA, Kolo PM, Mustapha AF, Adeyanju OA. Prevalence and clinical characteristics of headaches among undergraduate students in three tertiary institutions in Ilorin, Nigeria. Niger J Clin Pract 2017;20:1411-1416.ArticlePubMed
- 8. Oparah SK, Olose EO, Asibong UE, Ozomma SI. Migraine prevalence and impact among medical students of the university of Calabar, Southern Nigeria. World J Med Sci 2020;17:79-85.
- 9. Ekenze O, Ezeala-Adikaibe B, Orjioke C, et al. Prevalence and pattern of migraine, tension type headache and chronic daily headache among medical and nursing students in Enugu, South East Nigeria. Health 2018;10:1283-1293.ArticlePDF
- 10. Pilozzi A, Carro C, Huang X. Roles of β-endorphin in stress, behavior, neuroinflammation, and brain energy metabolism. Int J Mol Sci 2020;22:338.ArticlePubMedPMC
- 11. Misra UK, Kalita J, Tripathi GM, Bhoi SK. Is β endorphin related to migraine headache and its relief? Cephalalgia 2013;33:316-322.ArticlePubMedPDF
- 12. Ezeala-Adikaibe B, Onyekonwu C, Ijoma U, et al. Assessment of migraine disability using the migraine disability assessment questionnaire in young Nigerians. World J Neurosci 2018;8:411-422.ArticlePDF
- 13. Ali MW, Musami UB, Sa’ad FK, et al. Profile of migraine patients in a developing country: a multicentre study. SN Compr Clin Med 2020;2:1153-1157.ArticlePDF
- 14. Obafemi Awolowo University Teaching Hospitals Complex. A brief history of OAUTHC [Internet]. Obafemi Awolowo University Teaching Hospitals Complex; 2022 [cited 2022 Mar 28]. Available from: https://oauthc.gov.ng/about/about-oauthc
- 15. Jekel JF, Katz DL, Elmore JG, Wild DMG. Epidemiology, biostatistics and preventive medicine. 3rd ed. Saunders; 2007.
- 16. Bidari A, Ghavidel-Parsa B, Rajabi S, Sanaei O, Toutounchi M. The acute effect of maximal exercise on plasma beta-endorphin levels in fibromyalgia patients. Korean J Pain 2016;29:249-254.ArticlePubMedPMCPDF
- 17. Mohammed N, Allam H, Elghoroury E, Zikri EN, Helmy GA, Elgendy A. Evaluation of serum beta-endorphin and substance P in knee osteoarthritis patients treated by laser acupuncture. J Complement Integr Med 2018;15:20170010.ArticlePubMed
- 18. van Dongen RM, Zielman R, Noga M, et al. Migraine biomarkers in cerebrospinal fluid: a systematic review and meta-analysis. Cephalalgia 2017;37:49-63.ArticlePubMedPDF
- 19. Ren C, Liu J, Zhou J, et al. Low levels of serum serotonin and amino acids identified in migraine patients. Biochem Biophys Res Commun 2018;496:267-273.ArticlePubMed
- 20. Misra UK, Kalita J, Tripathi G, Bhoi SK. Role of β endorphin in pain relief following high rate repetitive transcranial magnetic stimulation in migraine. Brain Stimul 2017;10:618-623.ArticlePubMed
- 21. Song TJ, Chu MK. Exercise in treatment of migraine including chronic migraine. Curr Pain Headache Rep 2021;25:14.ArticlePubMedPDF
- 22. Suchting R, Colpo GD, Rocha NP, Ahn H. The effect of transcranial direct current stimulation on inflammation in older adults with knee osteoarthritis: a Bayesian residual change analysis. Biol Res Nurs 2020;22:57-63.ArticlePubMedPMCPDF
- 23. Choi HY, Lee CH. Can beta-endorphin be used as a biomarker for chronic low back pain? A meta-analysis of randomized controlled trials. Pain Med 2019;20:28-36.ArticlePubMed
- 24. Oshinaike O, Ojo O, Okubadejo N, Ojelabi O, Dada A. Primary headache disorders at a tertiary health facility in Lagos, Nigeria: prevalence and consultation patterns. Biomed Res Int 2014;2014:782915.ArticlePubMedPMCPDF
- 25. Birru EM, Abay Z, Abdelwuhab M, Basazn A, Sirak B, Teni FS. Management of headache and associated factors among undergraduate medicine and health science students of University of Gondar, North West Ethiopia. J Headache Pain 2016;17:56.ArticlePubMedPMCPDF
- 26. Raju S, Geetha S. Prevalence of migraine among medical students of a tertiary care teaching medical college and hospital in South India: a cross-sectional study. Natl J Physiol Pharm Pharmacol 2018;8:1377-1383.Article
- 27. Olugbake OA, Akinola AA, Ekiran OO. Knowledge and Use of over the counter analgesics among medical and nonmedical students of the University of Lagos. J Basic Soc Pharm Res 2019;1:37-45.Article
- 28. Puledda F, de Boer I, Messina R, et al. Worldwide availability of medications for migraine and tension-type headache: a survey of the International Headache Society. Cephalalgia 2024;44:3331024241297688.ArticlePubMedPDF
- 29. Dodick DW, Silberstein SD. Migraine. 3rd ed. Oxford University Press; 2016. p. 124.
- 30. Omogbiya AI, Anachuna KK, Umukoro EK, Moke EG, Nzei A. Academic-related stress and prevalence of migraine and tension-type headaches amongst undergraduates of Delta State University, Abraka, Nigeria. Res J Health Sci 2023;8:133-145.ArticlePDF
- 31. Halay S, Saror S, Abdalla AA, et al. Prevalence of migraine and trigger factors among adult rural Sudanese population 2018. Curr J Appl Sci Technol 2019;36:1-8.ArticlePDF
- 32. Rodríguez-Almagro D, Achalandabaso-Ochoa A, Obrero-Gaitán E, Osuna-Pérez MC, Ibáñez-Vera AJ, Lomas-Vega R. Sleep alterations in female college students with migraines. Int J Environ Res Public Health 2020;17:5456.ArticlePubMedPMC
- 33. Morgan I, Eguia F, Gelaye B, et al. Sleep disturbances and quality of life in Sub-Saharan African migraineurs. J Headache Pain 2015;16:18.ArticlePubMedPMCPDF
- 34. Oraby MI, Soliman RH, Mahmoud MA, Elfar E, ElMonem NAA. Migraine prevalence, clinical characteristics, and health care-seeking practice in a sample of medical students in Egypt. Egypt J Neurol Psychiatry Neurosurg 2021;57:26.ArticlePDF
- 35. Lipton RB, Manack Adams A, Buse DC, Fanning KM, Reed ML. A comparison of the Chronic Migraine Epidemiology and Outcomes (CaMEO) study and American Migraine Prevalence and Prevention (AMPP) study: demographics and headache-related disability. Headache 2016;56:1280-1289.ArticlePubMedPMCPDF
- 36. Yin JH, Lin YK, Yang CP, et al. Prevalence and association of lifestyle and medical-, psychiatric-, and pain-related comorbidities in patients with migraine: a cross-sectional study. Headache 2021;61:715-726.ArticlePubMedPDF
- 37. Alzahrani F, Hmoud M, Khayat H, et al. Knowledge of primary healthcare physicians about headache disorders: a cross-sectional study. Qual Prim Care 2016;24:83-86.
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-

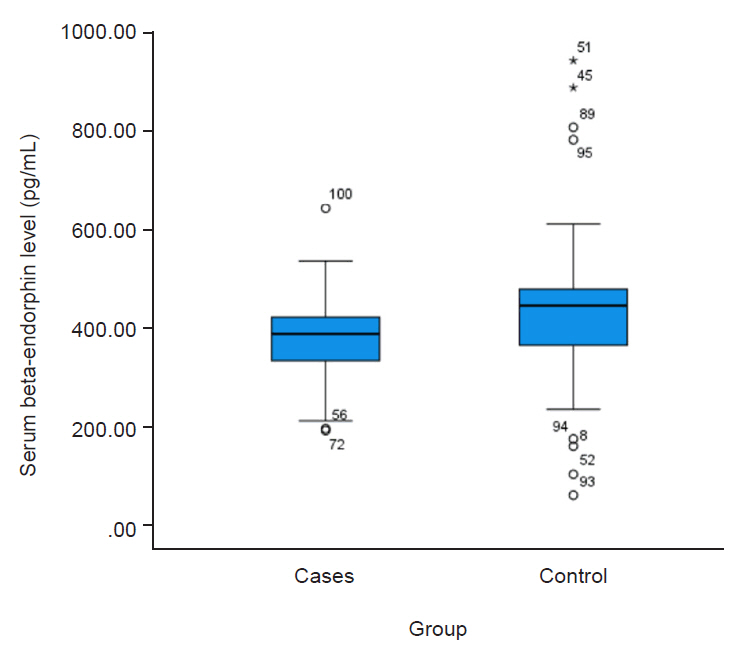
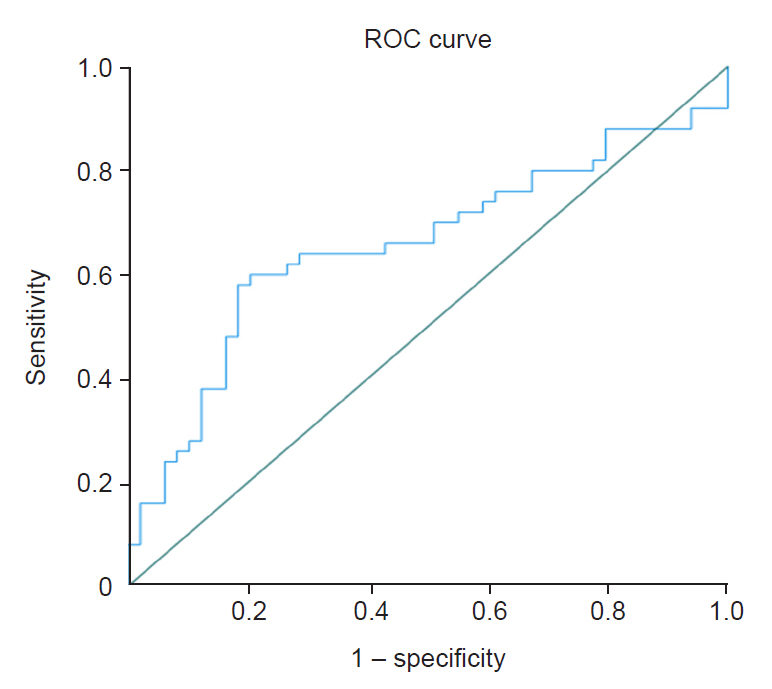



Figure 1.
Figure 2.
Figure 3.
| Variable | Category | Study group | Statistics | |
|---|---|---|---|---|
| Migraine headache group (n=50) | Healthy group (n=50) | |||
| Age (yr) | 22.0 (20.8–25.0) | 22.0 (21.0–24.0) | U=1,220.0, p=0.83 | |
| Sex | Male | 12 (24.0) | 12 (24.0) | χ2=0.05, p=0.82 |
| Female | 38 (76.0) | 38 (76.0) | ||
| Marital status | Single | 45 (90.0) | 47 (94.0) | Fisher’s=0.54, p=0.72 |
| Married | 5 (10.0) | 3 (6.0) | ||
| Body mass index (kg/m2) | 22.2 (19.4–26.0) | 21.3 (19.3–24.5) | U=1,124.0, p=0.38 | |
| Variable | Frequency |
|---|---|
| Average duration of headache per episode (hr) | 21.0 (6.3–48.0) |
| Duration since diagnosis of migraine headache (mo) | 30.0 (12.0–48.0) |
| Average cost of treatment of migraine headache (naira) | 500.0 (200.0–2,000.0) |
| Nausea | |
| No | 30 (60.0) |
| Yes | 20 (40.0) |
| Vomiting | |
| No | 39 (78.0) |
| Yes | 11 (22.0) |
| Photophobia/phonophobia | |
| No | 2 (4.0) |
| Yes | 48 (96.0) |
| Premonition signs | |
| No | 23 (46.0) |
| Yes | 27 (54.0) |
| Types of premonition signs (n=27) | |
| Sensory | 11 (40.7) |
| Visual | 8 (29.6) |
| Both | 5 (18.5) |
| Others | 3 (11.1) |
| Migraine prophylaxis | |
| No | 42 (84.0) |
| Yes | 8 (16.0) |
| Medication for prophylaxis (n=9) | |
| Propranolol | 1 (11.1) |
| Amitriptyline | 7 (77.8) |
| Amitriptyline+propranolol | 1 (11.1) |
| Medications for acute migraine | |
| Paracetamol | 21 (42.0) |
| Ergot preparation | 8 (16.0) |
| Aspirin | 5 (10.0) |
| Sumatriptan | 5 (10.0) |
| None | 1 (2.0) |
| Others | 10 (20.0) |
| Frequency of migraine headache | |
| Chronic migraine | 17 (34.0) |
| High frequency migraine | 4 (8.0) |
| Medium frequency migraine | 10 (20.0) |
| Low frequency migraine | 19 (38.0) |
| Variable | Intervention group | Statistics | |
|---|---|---|---|
| Migraine headache group (n=50) | Healthy group (n=50) | ||
| Serum beta-endorphin (pg/mL) | 385.4 (328.5–423.4) | 442.9 (357.5–477.6) | U=843,000, p=0.01 |
| AUC | p-value | 95% CI | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Cut off value (pg/mL) | |
|---|---|---|---|---|---|---|---|---|
| Beta-endorphin | 0.70 | 0.01 | 0.54–0.77 | 64.0 | 71.4 | 66.7 | 69.6 | 403.4 |
| Variable | Frequency of headache | Statistics | |||
|---|---|---|---|---|---|
| Chronic migraine | High-frequency migraine | Medium frequency migraine | Low frequency migraine | ||
| Serum beta-endorphin | 371.4 (299.5–415.8) | 380.2 (322.5–465.3) | 385.5 (315.2–435.3) | 387.4 (305.9–416.7) | H=0.255, p=0.968 |
Values are presented as median (interquartile range) or number (%). U, Mann-Whitney U-test.
Values are presented as median (interquartile range) or number (%).
Values are presented as median (interquartile range).
AUC, area under the curve; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value.
Values are presented as median (interquartile range).
Table 1.
Table 2.
Table 3.
Table 4.
Table 5.
TOP

