Finding the Sweet Spot between Medication Overuse and Underuse in Headache Medicine
Article information

Abstract
Medication-overuse headache (MOH) is a well-recognized secondary headache caused by the frequent use of acute symptomatic medications, particularly among patients with underlying primary headache disorders such as migraine. Medication-underuse headache (MUH) is a recently proposed conceptual framework describing the suboptimal use of indicated treatments, including underuse, delayed administration, poor adherence, or premature discontinuation, all of which may contribute to headache progression or chronification. Both conditions share pathophysiological substrates, including central sensitization, impaired descending pain modulation, and dysfunctional reward processing, which are rooted in dopaminergic mesocorticolimbic dysregulation and trigeminovascular sensitization. MUH may arise from fear of side effects, fear of withdrawal, poor adherence, or inadequate access to care and may lead to an escalating headache burden and increased reliance on acute treatments, potentially predisposing patients to MOH. Conversely, managing MOH without addressing underuse-related barriers may contribute to treatment resistance or relapse. Recent evidence suggests that calcitonin gene-related peptide (CGRP)-targeted monoclonal antibodies can achieve clinically meaningful improvement in MOH even without mandatory medication withdrawal, challenging the traditional assumption that detoxification is required for treatment response. MOH is also increasingly viewed as a multidimensional neurological and biobehavioral disorder, with preliminary neuroimaging data indicating that mindfulness-based interventions can modulate pain- and reward-related brain networks. This narrative review summarizes the clinical features and mechanisms of MOH and MUH and proposes a comprehensive management framework integrating patient education, structured lifestyle and mindfulness-based interventions, early initiation of preventive therapy, and CGRP-targeted treatments, with the aim of achieving therapeutic balance—not too much, not too little—and improving long-term outcomes.
INTRODUCTION
Medication-overuse headache (MOH) and medication-underuse headache (MUH) represent two ends of a spectrum concerning inadequate headache management. MOH, a well-characterized secondary headache disorder, occurs due to the excessive use of acute symptomatic medications in individuals who have an underlying primary headache disorder.1 This condition is well-documented in clinical practice, with numerous studies highlighting the consequences of overusing medications. Patients often find themselves caught in a cycle of increased headache frequency and severity, leading to a reliance on acute treatments. On the other hand, MUH is an emerging concept that refers to headache exacerbation resulting from insufficient or delayed use of appropriate acute or preventive treatments.2,3 It emphasizes that not only can overuse of medications lead to complications, but underuse can also significantly contribute to poor headache control.
Both MOH and MUH highlight the delicate balance required in headache therapy: not too much medication, not too little. Undertreatment may stem from patient reluctance, fear of potential adverse effects, or systemic barriers within healthcare settings,4 all of which can delay access to effective acute or preventive treatments. When headaches remain uncontrolled, patients increasingly rely on acute medications, and this reliance can ultimately contribute to the development of MOH. Therefore, it is imperative for both patients and healthcare providers to work collaboratively in addressing these challenges to ensure optimal headache management. Effective communication and education about the risks and benefits of medication use are vital for preventing both MOH and MUH, ultimately leading to improved patient outcomes.2,5
This review aims to explore MOH and medication underuse as potentially interconnected rather than opposing phenomena. A central argument is that the fear of withdrawal may itself perpetuate underuse and delay presentation, creating conditions for MOH development. Emerging evidence now challenges the requirement for mandatory medication withdrawal as a prerequisite for MOH treatment in non-opioid overuse. Calcitonin gene-related peptide (CGRP)-targeted monoclonal antibodies have demonstrated efficacy in both simple and complex non-opioid MOH regardless of whether withdrawal is undertaken. This represents a paradigm shift with direct implications for the management of patients who have previously failed or refused detoxification-based approaches. By synthesizing this updated evidence alongside the neurobiological basis of the medication underuse–MOH relationship, this review proposes a unified, patient-centered management framework that addresses both overuse and underuse through early preventive intervention, structured behavioral strategies, and individualized communication that reduces rather than reinforces stigma.
MEDICATION-OVERUSE HEADACHE: CURRENT STATUS AND CHALLENGES
1. Diagnosis
According to the International Classification of Headache Disorders, 3rd edition (ICHD-3),1 MOH is diagnosed when a patient experiences headache on 15 or more days per month and has used acute or symptomatic headache medications regularly for more than 3 months. The frequency threshold for medication overuse depends on the drug class: ≥10 days per month for triptans, ergotamines, opioids, and combination analgesics; and ≥15 days per month for non-steroidal anti-inflammatory drugs (NSAIDs) and simple analgesics like paracetamol.
MOH commonly occurs in patients with an underlying primary headache disorder, most frequently migraine or tension-type headache. Clinically, the headaches are often bilateral, dull, and pressing in quality, and frequently occur upon awakening. Patients often develop a characteristic pattern of escalating medication use, seeking short-term relief that paradoxically leads to worsening headache frequency and reduced responsiveness to acute treatments. Accurate diagnosis requires a detailed medication history, including prescription and over-the-counter drugs. Headache diaries are an essential tool for documenting headache frequency, medication intake, and timing, thereby assisting in diagnosis, patient education, and therapeutic planning.
2. Epidemiology and risk factors
MOH affects 0.5%–7.2% in the general population,6 with higher rates (up to 50%) observed among patients of specialized headache centers.7 Understanding these epidemiological trends is crucial for identifying at-risk patients and implementing preventive strategies effectively. Risk factors include high frequency of medication use, comorbid psychiatric disorders (depression and anxiety), physical inactivity, higher body mass index, and a history of chronic headache conditions.8-12 Addressing these risk factors can improve patient outcomes and reduce the prevalence of MOH.
3. Burden and societal impact
The global burden of MOH is significant and warrants attention due to its extensive impact on individuals and healthcare systems. MOH ranks 18th among all causes of Years Lived with Disability,13 highlighting its substantial contribution to disability worldwide.
According to the Eurolight study, the estimated annual economic burden of MOH in Europe alone reaches approximately €37 billion. This figure is largely attributed to productivity losses, which account for about 60% of the total costs, and healthcare utilization, which represents the remaining 40%.14
Patients suffering from MOH demonstrate a markedly poorer quality of life, with studies indicating that they may experience a quality-of-life score reduction of up to 30% compared to those with non-overused headache types. Patients with MOH often require more frequent healthcare resource utilization compared to non-MOH or potential medication overuse group; migraine-related inpatient (13.6% vs. 7.9%), emergency department visit (22.7% vs. 18.5%), and evaluation and management visit (3.1 vs. 2.1).15 Approximately 50% of patients with MOH report more than 20 days of work loss in the past 3 months, substantially higher than patients with tension-type headache (around 3%) or migraine (approximately 10%–15%).16 The challenges faced by patients with MOH are often exacerbated by comorbidities such as anxiety and depression, which are prevalent in up to 50% of these individuals.
Even with treatment, the process can be quite challenging. Standard treatment emphasizes withdrawal of overused medications, followed by the introduction of preventive therapy. However, this approach is often difficult due to withdrawal symptoms, patient resistance, and high relapse rates—reported to be up to 45% within the first year.17 These challenges underscore the need for proactive, individualized prevention strategies that begin well before overuse develops.
The burden of MOH is therefore both clinical and economic, underscoring the need for improved diagnostic and management strategies.
4. Pathophysiology of medication-overuse headache: a biobehavioral framework
Understanding the neurobiological basis of MOH is essential for clinicians, both to explain disease progression to patients and to select rational treatment strategies. MOH pathophysiology involves three interconnected mechanisms: dysregulation of the brain’s reward system, trigeminovascular sensitization, and maladaptive cortical neuroplasticity. These mechanisms provide the biological rationale for treatment approaches that go beyond simple medication withdrawal, and may also help explain how inadequate treatment can set the stage for subsequent overuse.18,19
The mesocorticolimbic dopaminergic system—originating in the ventral tegmental area and projecting to the nucleus accumbens (mesolimbic pathway) and prefrontal cortex (mesocortical pathway)—is the primary neuroanatomical substrate of MOH’s reward-related dysfunction.20-22 Structural magnetic resonance imaging studies demonstrate increased gray matter volume in the ventral striatum of MOH patients compared with healthy controls, a region implicated in reward and addiction.20-23 Functional neuroimaging reveals impaired representation of long-term reward values in the dorsomedial prefrontal cortex and ventral striatum, with altered connectivity at rest.20-22 Critically, patients with MOH exhibit impulsive decision-making and Pavlovian conditioning. Environmental cues associated with prior medication use can independently trigger craving and drug-seeking behavior, reinforcing compulsive patterns of analgesic use even without genuine therapeutic need. These features closely parallel those of substance use disorders, sharing genetic polymorphisms in dopaminergic pathways and behavioral phenotypes including ritualized drug use and psychological dependence. Importantly, recent evidence reconceptualizes MOH as a multidimensional neurological biobehavioral disease rather than a moral failure or simple habit, a distinction with significant implications for how clinicians communicate with and educate patients.
The trigeminovascular system provides the second major mechanism. Activation of first-order trigeminal neurons through inflammatory mediators and neuropeptides including CGRP and substance P leads to peripheral sensitization. Continued activation promotes central sensitization, in which second- and third-order neurons generate pain signals without requiring peripheral input. Chronic analgesic or triptan exposure appears to lower the activation threshold of this system: triptans increase circulating CGRP levels with prolonged use, while opioids induce CGRP overexpression in dorsal root ganglion neurons and promote glial-mediated neuroinflammation. Acetaminophen overuse increases susceptibility to cortical spreading depression (CSD). These drug-specific mechanisms explain why even agents considered “safe” for acute use can contribute to MOH when used excessively, and why triptans precipitate MOH more rapidly (mean 1.7 years) than simple analgesics (mean 4.8 years).19 The endocannabinoid system (ECS) normally provides tonic inhibition of pain and modulation of neuroinflammation through its principal lipid mediators, anandamide and 2-arachidonoylglycerol, acting on CB1 and CB2 receptors. Reduced endocannabinoid levels have been documented in MOH patients, suggesting ECS dysfunction contributes to the maintenance of the sensitized state.24
Altered cortical excitability represents the third mechanism. Preclinical studies show that chronic analgesic or sumatriptan exposure lowers the CSD threshold and increases CSD frequency, the electrophysiological event thought to initiate migraine with aura. Increased c-fos expression in the trigeminal nucleus caudalis following paracetamol exposure indicates enhanced nociceptive pathway activation.25 Together, these three mechanisms create a self-reinforcing cycle: medication use worsens neurobiological vulnerability, making headaches easier to trigger and acute medications less effective. It is important to note that medication underuse does not carry a distinct pathophysiology separate from that of MOH. Both overuse and underuse of acute medications, as well as insufficient preventive therapy, converge on the same final pathway of central sensitization. The routes might differ: in MOH, repeated medication exposure directly sensitizes the trigeminovascular system and dysregulates reward circuitry, whereas in underuse, inadequately treated attacks allow uninterrupted trigeminal nociceptive input to progressively reinforce central sensitization. This underscores the neurobiological window within which early and effective acute treatment may prevent sensitization from becoming entrenched.3 This framework may potentially predispose undertreatment to overuse: when effective acute or preventive therapy is not initiated promptly, progressive central sensitization lowers the pain threshold, increasing both headache frequency and medication-seeking behavior (Figure 1). Further prospective longitudinal studies are warranted to establish the causal relationship between treatment underuse and MOH development.
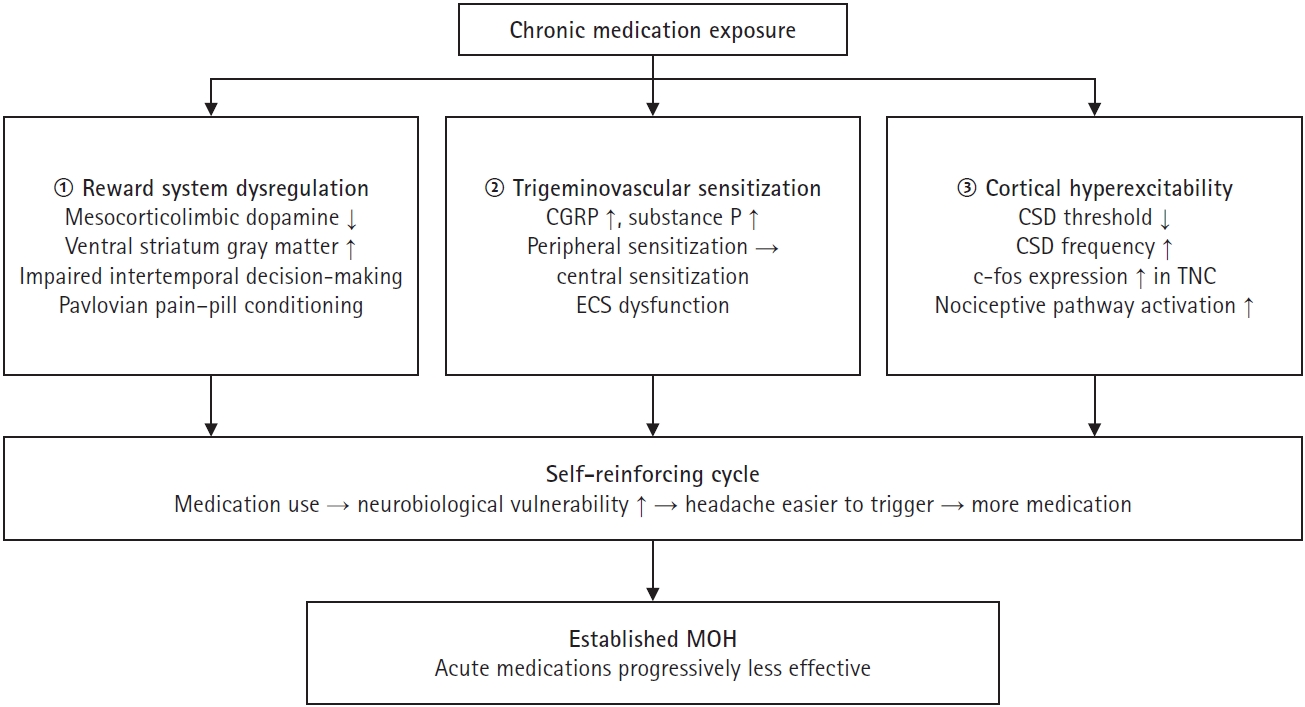
Pathophysiological mechanisms of MOH.
CGRP, calcitonin gene-related peptide; ECS, endocannabinoid system; CSD, cortical spreading depression; TNC, trigeminal nucleus caudalis; MOH, medication-overuse headache.
MEDICATION-UNDERUSE HEADACHE: A PROPOSED FRAMEWORK FOR HEADACHE CHRONIFICATION
MUH describes the suboptimal application of indicated headache treatments—encompassing underutilization, delayed administration, poor adherence, or premature discontinuation of acute or preventive therapies.2 It is important to emphasize that MUH is not currently a formal diagnostic entity in the ICHD-3, and its direct causal role in headache chronification has not yet been established in prospective studies. Nonetheless, it provides a clinically useful framework for understanding patterns of inadequate treatment that may contribute to poor headache control and potentially increase susceptibility to MOH. These patterns are typically not attributable to a single failure, but to the cumulative effect of multiple deficiencies in headache management spanning patient behavior, provider decisions, and healthcare system limitations.
1. Inadequate acute treatment
Timely administration of effective acute treatment is essential for halting migraine attacks and preventing central sensitization. However, several patterns of underuse contribute to MUH in the acute treatment phase.
1) Ineffectiveness of acute medications
When acute treatments fail to abort a migraine attack effectively, this suboptimal response is associated with an increased risk of migraine chronification. The American Migraine Prevalence and Prevention (AMPP) study found that patients with “very poor” or “poor” acute treatment response had a higher rate of conversion to chronic migraine over 1 year compared to those with “maximal” response (6.8%, 4.4%, and 1.9%, respectively).26 A Japanese disease-specific program showed an association between triptan unresponsiveness with more frequent headache days.27 These studies emphasized the need for timely and effective intervention.
2) Improper timing of administration
Delayed use of acute therapy, defined as waiting until pain is moderate to severe, reduces efficacy and increases the likelihood of headache persistence. This is often due to misunderstanding of optimal treatment timing or hesitancy to medicate early. The TEMPO study showed that early dosing of almotriptan (<1 hour after headache onset) resulted in a significantly higher pain-free rate than late dosing (52.8% vs. 30.2%, p<0.01).28 Similar result was obtained from the Act when Mild (AwM) trial showing that treating when the pain is mild and within 1 hour of headache onset leads to better outcomes (53% vs. 38%, p=0.03).29 The PRODROME trial showed that ubrogepant taken at the first qualifying prodomal symptom resulted in a higher absence rate of moderate or severe headache within 24 hours compared to placebo.30 If the acute treatment was delayed after central sensitization has occurred, patients might experience insufficient pain relief and persistent disability, potentially leading to migraine progression.
3) Adverse effects and intolerability
Adverse effects (such as chest discomfort from triptans or ergotamine, and gastrointestinal upset from NSAIDs) and poor tolerability are significant barriers to the adequate use of acute treatment. The Chronic Migraine Epidemiology and Outcomes (CaMEO) study found that safety and intolerability accounted for 24.9% of discontinuations.31 Another survey also demonstrated that 29% of triptan users discontinued their medications due to side effects.32
4) Fear of withdrawal and stigma as drivers of underuse
A particularly underrecognized barrier to appropriate headache management is the fear of withdrawal itself. Many patients who have been informed—or who have personally experienced—that stopping overused medications causes a rebound worsening of headache become reluctant to seek specialist care, reduce their medications, or initiate preventive therapy. This fear perpetuates continued overuse, or conversely, drives avoidance of care altogether, leaving the underlying migraine biology unaddressed. The result is a vicious cycle: inadequate treatment leads to more frequent headaches, which leads to more acute medication use, which reinforces the fear of stopping.
The language surrounding MOH has historically compounded this problem. The term “detoxification”, widely used to describe withdrawal from overused medications, carries strong connotations of addiction and moral failure. This stigma deters patients from acknowledging their pattern of use and engaging with treatment. Emerging expert consensus suggests that more precise and less stigmatizing terminology should be adopted in clinical practice: the term “withdrawal” should be reserved for patients overusing opioids or barbiturates, where physiological dependence is a genuine concern; for patients overusing simple analgesics or triptans, “pausing medication” more accurately describes what is required and avoids unnecessary alarm. This terminological shift is not merely semantic—it has practical implications for patient engagement, adherence to treatment plans, and willingness to initiate preventive therapy. Clinicians who frame the conversation around “pausing” rather than “detoxifying” are more likely to overcome the fear barrier and facilitate the therapeutic transitions necessary to address the underuse-to-overuse cycle.18
2. Inadequate preventive treatment
Preventive therapy is critical for patients experiencing frequent headaches (typically ≥4–8 days/mo), yet it remains significantly underused and inconsistently applied in clinical practice worldwide. Only 22%–32% of the patients who are eligible for preventive treatment from the headache center actually used preventive treatment.33,34 From a prospective nationwide MOH registry in Korea (Registry for Load and Management of Medication Overuse Headache, RELEASE), 7% of the patients diagnosed with MOH still did not receive appropriate preventive therapy, even though headache specialists had recommended preventive options.8 Despite established guidelines recommending preventive treatment for patients with recurrent or disabling headaches, studies show that a large proportion of eligible patients never receive appropriate prophylaxis, and those who do often discontinue it prematurely.
1) Difficult to initiate
Preventive treatment initiation can be challenging due to various barriers, including patient reluctance, lack of awareness about treatment options, and concerns regarding potential side effects. Both physicians and patients may not recognize headache progression or chronification. Some patients only report their “severe” headaches, may overlook the importance of addressing milder episodes, which can also contribute to overall headache burden. Physicians, especially in busy primary care settings, may not probe deeply into headache diaries or conduct structured interviews, resulting in missed opportunities to initiate preventives in a timely fashion. Many patients are concerned about the potential adverse effects such as weight gain, cognitive impairment, over-sedation, or dependency on preventive medications, which may prevent initiation and perpetuate the cycle of headache exacerbation.
2) Difficult to continue
The difficulty of continuing preventive treatment can largely be divided into two categories; 1) inadequate dosing or titration, and 2) premature discontinuation. If physicians did not have enough experience with preventive medications, they may prescribe inadequate doses or fail to properly titrate the medication, leading to suboptimal efficacy. After reaching the therapeutic dose, both physicians and patients should maintain preventive treatment for at least 3–6 months to assess its effectiveness. However, it is not easy to achieve this, as many patients experience adverse effects, perceive a lack of immediate improvement, or modest efficacy of traditional preventive treatment.
These barriers play a significant role in the underutilization of preventive therapy, which is essential for alleviating the burden of headaches. Focused educational initiatives targeting both patients and healthcare providers are therefore needed to raise awareness and improve adherence to preventive therapy.
3. Lack of education and lifestyle intervention
Effective headache management necessitates a comprehensive approach that integrates not only pharmacological strategies but also patient education and structured lifestyle interventions. Despite their well-documented benefits, these non-pharmacological components are frequently overlooked in both primary and specialized care settings, contributing to suboptimal outcomes and increased risk of headache progression. An additional barrier to appropriate treatment is the widespread misconception that medications cannot alter the natural course of migraine. While no formally approved disease-modifying treatments currently exist for migraine, evidence clearly demonstrates that inadequate treatment can facilitate central sensitization and contribute to disease progression and chronification. Correcting this misconception is therefore an essential component of patient education.
Patient education plays a pivotal role in empowering individuals to engage in self-management and make informed decisions regarding treatment. A thorough understanding of headache pathophysiology, recognition of early symptoms, and differentiation between headache subtypes (e.g., migraine vs. tension-type headache) are essential. Early intervention with appropriate medications is significantly more effective than delayed treatment, yet many patients initiate therapy too late in the attack due to lack of awareness or misconceptions about medication use. Enhancing patient understanding of the importance of prompt and appropriate treatment timing can reduce headache severity and prevent chronification.
Lifestyle modifications represent another cornerstone of non-pharmacologic management. Consistent sleep schedules, regular meal timing, adequate hydration, stress reduction techniques, and routine physical activity have all been shown to reduce headache frequency and severity in susceptible individuals. While these strategies may appear basic, their sustained implementation requires education, motivation, and follow-up support from healthcare providers.
Among non-pharmacological approaches, mindfulness-based interventions have shown preliminary promise and are beginning to attract neurobiological investigation. A small randomized clinical trial in 34 patients with chronic migraine and MOH found that a structured six-session mindfulness program emphasizing meditation, awareness, and acceptance was associated with measurable changes in neurochemical connectivity on functional imaging after 1 year.35 Specifically, mindfulness training enhanced serotonin-enriched connectivity in the caudate nucleus and nucleus accumbens, and increased dopamine-enriched connectivity in the right insula—all regions implicated in affect regulation, reward processing, cognitive pain control, and pain modulation. These findings suggest that mindfulness may modulate neurochemical networks involved in pain regulation and the conditioned association between pain anticipation and medication intake. However, given the small sample size and single-centre design of the available study, these neuroimaging findings should be interpreted with caution and require replication in larger trials before definitive conclusions can be drawn. Nonetheless, given the favorable safety profile and the biological plausibility of the observed effects, mindfulness-based programs may serve as a reasonable adjunct to pharmacological treatment and patient education, particularly in patients with MOH where behavioral factors are prominent.18,35
The use of headache diaries or digital tracking tools further enhances patient engagement and clinical decision-making. Systematic recording of headache frequency, intensity, duration, medication use, and potential triggers helps identify patterns that inform personalized management plans. These tools also facilitate monitoring of adherence, medication overuse, or underuse, allowing for timely intervention.
In the absence of structured education and behavioral support, patients may feel disempowered and unprepared to manage their condition effectively. This can result in inconsistent medication use, avoidance of preventive therapy, and increased reliance on acute treatments—all of which contribute to the risk of developing MOH. Therefore, it is essential to integrate education and lifestyle counseling into routine clinical practice, and structured programs and multidisciplinary support are recommended to ensure patients receive comprehensive, evidence-based care that addresses both medical and behavioral determinants of headache burden.
THE MEDICATION UNDERUSE–MEDICATION-OVERUSE HEADACHE RELATIONSHIP: A CLINICAL PERSPECTIVE
The relationship between MOH and MUH is complex and, while not yet formally established, is clinically plausible given their shared pathophysiological substrates (Figure 2). Patients may experience these patterns along a shared clinical trajectory, with one state potentially facilitating transition to the other over time. A patient who avoids or delays effective treatment may experience progressive central sensitization, lowering the pain threshold and increasing headache frequency. As headache days accumulate and quality of life deteriorates, the patient resorts to increasingly frequent acute medication use. Over months, this rational short-term response may cross the threshold into MOH. Conversely, a patient attempting to reduce overuse who fears withdrawal may continue overusing medications, unable to engage with preventive therapy, thereby remaining trapped in the cycle.
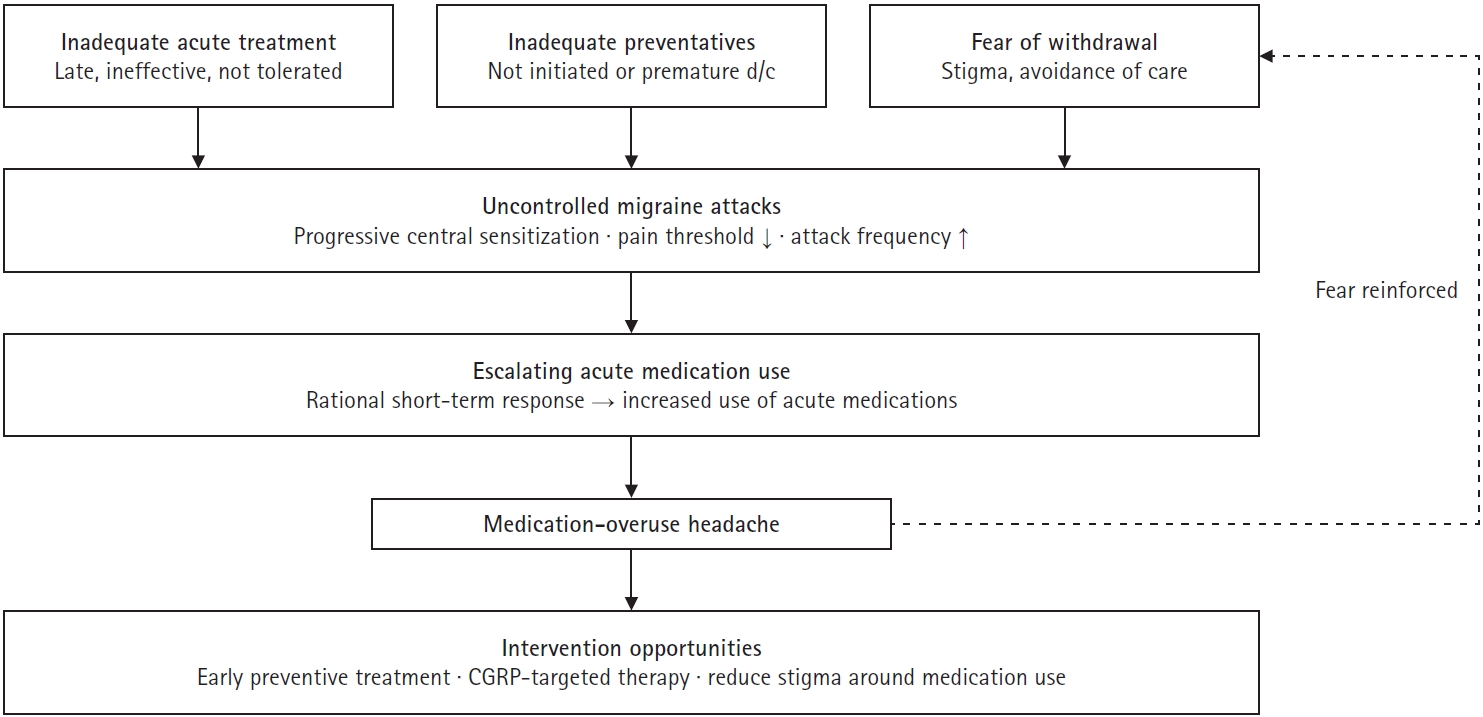
From medication underuse to medication overuse: vicious cycle in headache management.
d/c, discontinuation; CGRP, calcitonin gene-related peptide.
From a neurobiological standpoint, both MOH and MUH may share and mutually reinforce the mesocorticolimbic reward system dysregulation, trigeminovascular sensitization, and maladaptive cortical neuroplasticity (described in the Pathophysiology of MOH: A Biobehavioral Framework section). Central sensitization, once established, does not resolve spontaneously; it requires either effective preventive treatment or relief from the ongoing sensitizing stimulus (medication overuse). Insufficient treatment may permit central sensitization to develop and deepen, generating the neurobiological substrate into which MOH develops. Once MOH is established, the dysregulated mesocorticolimbic reward system further impairs the patient’s capacity to reduce medication use voluntarily. Pavlovian conditioning between environmental pain cues and medication intake means that even the anticipation of a headache can trigger compulsive medication-seeking behavior. This is neurobiologically driven, not simply a matter of willpower or patient compliance. This reframing has significant implications for clinical communication—patients should be informed that their difficulty stopping medications reflects brain-level conditioning that can be effectively addressed with evidence-based treatment, not a character flaw.
Neuroimaging findings illustrate dysfunctional reward processing in MOH. The subjective value of long-term rewards, such as headache freedom achieved through preventive therapy, is weaker in MOH patients compared with controls, while short-term relief from acute medication is overweighted. This impaired intertemporal decision-making makes it intrinsically difficult for patients caught in the MOH state to choose the longer-term benefit of preventive treatment over the immediate relief of another analgesic dose. Understanding this neurobiological reality informs both patient counseling and the strategic value of CGRP-targeted therapies, which can restore headache control without requiring patients to first navigate this impaired reward landscape through willpower alone.
Recognizing this potential relationship allows clinicians to identify at-risk patients earlier and implement more targeted interventions. The most effective time to intervention is before central sensitization becomes entrenched. Early and appropriate acute therapy, combined with timely initiation of preventive treatment during the pre-overuse phase, may halt progression to MOH. Even in established MOH, modern treatment approaches including CGRP-targeted therapies and, potentially, behavioral interventions such as mindfulness offer pathways to recovery that do not require the patient to first undergo aversive withdrawal, thereby addressing one of the principal barriers that keeps patients trapped in a cycle of overuse.
COMPREHENSIVE MANAGEMENT STRATEGY: AN INTEGRATED APPROACH TO MEDICATION-OVERUSE HEADACHE AND MEDICATION-UNDERUSE HEADACHE
Effective prevention and management of both MOH and medication underuse requires an integrated approach emphasizing early detection, patient empowerment, and individualized pharmacologic and behavioral interventions. Clinicians must balance assertive prevention with clear patient communication and education.
1. Patient education and self-monitoring
Many patients have fears regarding medication use, dependency, long-term toxicity, and adverse effects such as weight gain or cognitive fog. These fears are often amplified by inadequate counseling or negative past experiences. Clinicians must proactively dispel myths and clarify the distinct goals of acute and preventive medications. Patients should be instructed to record all headache days, including those on which they chose not to take acute medication, rather than medication-use days alone. Advising patients to limit acute medication use to fewer than 8–10 days per month may inadvertently lead some patients to endure pain without treatment and underreport their true headache frequency. Patients should also be encouraged to maintain structured headache diaries, including the documentation of even mild headache episodes. These records help identify trends, guide treatment timing, and offer insight into medication efficacy. Mild or subclinical attacks are especially important to capture, as they often precede more severe exacerbations. Emphasizing the value of daily tracking supports patient engagement and helps clinicians adjust therapy based on accurate, real-time data.
2. Optimizing provider-patient communication and personalized care
Given the lack of objective biomarkers in headache disorders, physicians must rely heavily on patients’ subjective reports. Thus, effective communication is critical. Clinicians should actively listen for early cues of underuse or overuse, validate patient experiences, and tailor interventions accordingly. Importantly, side effects can be reframed constructively; for example, sleepiness induced by amitriptyline may be leveraged to improve insomnia, while weight gain from certain beta-blockers may warrant dietary counseling and closer monitoring rather than immediate discontinuation.
3. Integrating calcitonin gene-related peptide-targeted therapies
The advent of CGRP-targeted therapies represents a paradigm shift not only in migraine prevention, but specifically in the management of MOH. Agents such as erenumab, fremanezumab, galcanezumab, and atogepant have demonstrated robust efficacy even in patients with established medication overuse. Critically, emerging evidence has challenged the longstanding assumption that medication withdrawal is a prerequisite for treatment response. In a real-world study of 200 patients with chronic migraine and MOH, treatment with CGRP-targeting monoclonal antibodies produced substantial reductions in headache frequency, intensity, and acute medication use regardless of whether formal withdrawal was undertaken. This finding was also observed even in “complex” MOH defined by psychiatric comorbidities, prior relapse, or near-daily intake of multiple medications.36 This aligns with the only dedicated randomized controlled trial to date, in which monthly erenumab (140 mg) achieved MOH remission in patients with chronic migraine and non-opioid MOH without any withdrawal strategy.37 These findings have profound practical implications: for patients overusing non-opioid medications who are fearful of withdrawal, who have previously failed detoxification attempts, or who are currently underusing treatment and at risk of progression, CGRP-targeted therapies can be initiated without mandatory withdrawal as a primary strategy. It must be noted that this withdrawal-free approach applies only to non-opioid MOH. For patients overusing opioids or barbiturates, physiological dependence remains a genuine concern, and structured withdrawal under appropriate supervision is still recommended. As newer agents such as rimegepant and eptinezumab become accessible in South Korea and other settings, clinicians should remain informed and open to integrating these options into routine care for both prevention and MOH management.
Early use of CGRP-targeted therapies can help prevent escalation to established MOH and mitigate the consequences of prolonged undertreatment, particularly in patients with high-frequency episodic or chronic migraine at risk of progression or early MOH. For patients already in non-opioid MOH, initiating CGRP-targeted therapy without requiring withdrawal removes a key barrier to engagement and allows neurobiological recovery from sensitization to proceed in parallel with headache frequency reduction. By combining these pharmacologic advances with structured behavioral and non-pharmacological interventions, healthcare systems can achieve more stable, long-term headache control and reduce the burden across both extremes of medication mismanagement.
CONCLUSION
Headache management requires balance. Both excessive reliance on acute medications and failure to use preventive therapies appropriately can worsen outcomes. MOH and medication underuse should not be seen as isolated or opposing extremes but as potentially interrelated components of headache chronification. Both share neurobiological mechanisms including central sensitization, trigeminovascular sensitization, and mesocorticolimbic reward dysregulation. Understanding these mechanisms helps explain why the path to MOH is not simply a matter of patient behavior, but may reflect brain-level adaptations that are amenable to targeted treatment.
Recognizing the MOH-MUH continuum and proactively addressing medication underuse patterns that may precede overuse is essential for halting headache progression, reducing healthcare burden, and improving patient quality of life. Clinicians who integrate early pharmacological intervention, patient-centered communication, structured behavioral support, and awareness of the bidirectional relationship between underuse and overuse will be best positioned to interrupt headache progression and achieve durable outcomes for their patients.
Notes
AVAILABILITY OF DATA AND MATERIAL
Not applicable.
AUTHOR CONTRIBUTIONS
Conceptualization: HKP; Writing–original draft: HKP; Writing–review & editing: HKP.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING STATEMENT
None.
ACKNOWLEDGMENTS
None.