Natural Diagnostic Classes of Headache Disorders: Latent Class Analysis of a Population-Based Study
Article information

Abstract
Purpose
The International Classification of Headache Disorders, 3rd edition (ICHD-3), diagnoses headache based on combinations of clinical symptoms. Overlap is common, and symptom variability complicates diagnosis. We evaluated natural classes of headache disorders using a statistical approach and compared them with ICHD-3 diagnostic categories.
Methods
Data from a nationwide, population-based web survey on headache and sleep conducted in South Korea (n=3,030) were analyzed. Participants with headache (n=1,938) were included. Latent class analysis was performed using categorical ICHD-3 diagnostic criteria to identify distinct classes. The characteristics of each class and the distribution of ICHD-3 primary headache diagnoses were examined.
Results
Nine classes were identified, comprising 626, 54, 248, 148, 187, 143, 79, 61, and 392 individuals. Three classes were tension-type headache (TTH)–like: Class 1 was male-dominant mild bilateral TTH, Class 8 represented classic, severe TTH, and Class 9 was mild unilateral TTH. Class 4 showed a typical migraine phenotype and contained most migraine cases. Classes 5 and 6 were dominated by probable migraine (PM) and differed mainly in sensory sensitivity and disability, which were higher in Class 6. Classes 2, 3, and 7 were categorized as “other headache.” Class 2 had the highest prevalence of medication-overuse headache (MOH), whereas Class 3 was characterized by mild headache with nausea. Class 7 showed a mixed-type profile with prominent photophobia. Severity and central sensitization markers were key classifiers.
Conclusion
Latent class analysis identified nine clinically distinct headache classes. PM was clearly distinct from both TTH and migraine. One subtype of “other headache” showed the highest MOH burden.
INTRODUCTION
The diagnosis of headache disorders relies on clinical criteria based on International Classification of Headache Disorders, 3rd edition (ICHD-3).1 Although there is well established pathophysiologic evidence of different headache diagnosis, there being no biomarker, the diagnosis is based on a combination of clinical profiles. However, substantial variability in the time between attacks is often observed in individual patients. Prior studies of natural subgroups of migraine and tension-type headache (TTH), as well as concurrent ICHD-3 diagnoses, have demonstrated heterogeneity and overlap between several headache disorders.2-7 Also, current diagnosis of headache only allows definitive diagnosis, but frequently, there are occasions when a definite diagnosis and probable diagnosis are both present, such as those with definite diagnosis of TTH, but also who fit for the diagnosis of probable migraine (PM). In Korea where prevalence of PM is higher than migraine, the diagnostic and treatment challenges are greater, thus delaying patient diagnosis and appropriate treatment.8 Statistical analysis of ICHD-3 criteria revealed coexisting diagnoses5, suggesting alternative diagnostic classifications for headache disorders.
Statistical methods have been utilized to identify different subgroups of migraine amd TTH based on clinical characteristics or comorbidities.2-4 Identifying such subgroups could enhance our understanding of disease heterogeneity and support more precise classification and management, thereby improving precision medicine. Latent class analysis (LCA) is a model-based, probabilistic approach that identifies unobserved (latent) subgroups from a set of categorical variables and has been previously applied to classify headache disorders.2-4,9 Beyond the categorical structure of the data, LCA is particularly suitable for headache research because it allows for the identification of clinically interpretable phenotypic patterns while accounting for uncertainty in class membership. Given that the ICHD-3 diagnostic criteria consist largely of categorical symptom-based indicators, we applied LCA to a population-based sample of headache disorders to identify natural headache classes and to compare these data-driven classes with ICHD-3 diagnosis.
MATERIALS AND METHODS
1. Ethical approval
The present study was approved by the Institutional Review Board of the Severance Hospital, Yonsei University (approval no. 2022-2189-003). This study was conducted in accordance with the principles of the Declaration of Helsinki, and all participants provided written informed consent.
2. Data
We used the data of Circannual Change in Headache and Sleep (CHASE) study for the analysis. The CHASE study is a web-based survey on headache and sleep that was designed to represent the Korean population. The acquisition of the study was described previously in detail.10 In short, the study was a web-based questionnaire supported by Hankook Research (Seoul, Republic of Korea). An email with link to the survey was sent to those selected by a two-stage stratified clustered random sampling method proportional to population distribution. The survey included baseline and follow-up evaluation every 3 months for a year. This study is a cross-sectional analysis of the baseline data conducted in October 2020. Individuals aged 20–59 years were included according to socioeconomic and demographic strata derived from the 2015 National Statistical Office Population and Housing Census.11 Those with history of COVID-19 infection were excluded. The estimated sampling error was ±1.8%.
3. Diagnosis of headache disorders
The Headache disorders were diagnosed using a validated web-based questionnaire based on ICHD-3 with reasonable sensitivity (92.6, 85.0, and 78.4), specificity (94.8, 92.9, and 98.4), and accuracy (93.8, 91.0, and 92.6), for migraine, PM, and TTH, respectively.12 The diagnosis was based on ICHD-3 criteria for Migraine without aura (code 1.1), PM without aura (code 1.5.1), and infrequent episodic TTH (code 2.1).1 PM was diagnosed only when there was no definite headache diagnosis and there was no overlap in the diagnosis of headaches. Headache duration in this study was assessed as “Please specify the duration of your most severe headache in the past 3 months. If you use acute (rescue) medication, report the duration as if you had not taken it.” The frequency criteria was not used to differentiate episodic and chronic headache but was analyzed as a separate variable. The diagnostic criteria for migraine with aura (code 1.2) requires diagnosis of fulfilling criteria for migraine without aura. Visual aura was assessed by the Visual Aura Rating Scale, with score of ≥3 defined as having visual aura. Migraine in this study refers to migraine with and without aura, and chronic migraine. In the same way, TTH in this study refers to infrequent episodic TTH, frequent episodic TTH (code 2.2), and chronic TTH (code 2.3). PM stands for PM without and with aura (code 1.5.2). Those with headache not diagnosed as migraine, PM, and TTH were classified as other headache disorder. Medication-overuse headache (MOH) was diagnosed using ICHD-3 criteria.
4. Impact and disability of headache, cutaneous allodynia
The impact of headache disorder was assessed using the Headache Impact Test-6 (HIT-6).13 The disability of headache was assessed using the Migraine Disability Assessment (MIDAS).14 The higher scores indicated more impact and disability.
Allodynia Symptom Checklist-12 (ASC-12) questionnaire was used to assess cutaneous allodynia (CA).15 ASC-12 score ≥3 indicates CA.
5. Assessment of comorbid symptoms: anxiety, depression, fibromyalgia, and sleep related indices
Anxiety was assessed with General Anxiety Disorder-7 (GAD-7).16 GAD-7 scores ≥8 was defined as anxiety. Depression was assessed with Patient Health Questionnaire (PHQ-9), PHQ-9 scores ≥10 indicated depression.17 Fibromyalgia syndrome (FMS) was assessed using widespread pain index and symptoms severity score, and was diagnosed using 2016 criteria of American College of Rheumatology.18 Excessive daytime sleepiness (EDS) was assessed with Epworth Sleepiness Scale score ≥11 indicating EDS.19 Quality of sleep was assessed using the Pittsburgh Sleep Quality Index, ≥8.5 indicating poor sleep quality.20 Insomnia was assessed using Insomnia Severity Index (ISI), with ISI ≥15 defined as clinical insomnia.21
6. Statistical analysis and latent class analysis modeling
LCA is a probabilistic analytic method deriving ‘latent’ classes by stratifying observations with similar response from latent mixture of underlying distributions from categorical variables.9 Observations that are similar, though not identical, are clustered into the same class, thereby identifying subgroups with distinct characteristics. We conducted LCA using the ‘poLCA’ package 1.6.0.1 version in R, frequently used for LCA.22 As the categorical variables, the major variables used for diagnosis in ICHD-3 were selected; headache intensity, unilateral location, pulsating quality, aggravation by routine physical activity, nausea, vomiting, photophobia, and phonophobia were included. Headache frequency per month was categorized into four classes (<2, ≥2 to <8, ≥8 to <15, and ≥15 days). Headache duration was categorized as <30 minutes, ≥30 minutes to <4 hours, ≥4 hours to ≤72 hours, >72 hours to ≤7 days, and >7 days. Model quality was assessed using posterior class membership probabilities and class-conditional item-response probabilities. The local independence assumption was assessed by examining bivariate residuals for all pairs of observed indicators following model estimation (Supplementary Table 1, available online). To avoid convergence to local maxima during the expectation–maximization algorithm, each model was estimated 20 times using different sets of random starting values. Model fit was evaluated using the log-likelihood, Akaike information criterion (AIC), Bayesian information criterion (BIC), relative entropy, and the Lo–Mendell–Rubin likelihood ratio test (LMR-LRT).23,24 The optimal number of latent classes was determined based on a combination of statistical indices and clinical interpretability. Lower AIC and BIC values indicated better model fit, whereas higher relative entropy and a significant LMR-LRT supported superior classification performance. Descriptive statistics were summarized as means with standard deviations or medians with interquartile ranges for continuous variables, depending on their distribution, and as counts with percentages for categorical variables. To compare clinical and demographic characteristics across latent classes, one-way analysis of variance or the Kruskal–Wallis test was applied for continuous variables, depending on normality assumptions. Normality was assessed using the Shapiro–Wilk test and visual inspection of histograms and Q–Q plots. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. Multiple comparisons were adjusted using the Bonferroni correction. All statistical analyses were performed using R software (version 4.4.1; R Foundation for Statistical Computing). Two-sided p-values <0.05 were considered statistically significant.
RESULTS
1. Participants with headache
Of 91,153 individuals invited by email, 10,699 consented to participate. Among them, 6,215 discontinued the survey, 1,075 declined enrollment after screening, and 379 were excluded because a quota had been reached, leaving 3,030 participants who completed the survey (Figure 1). The distributions of age, sex, and residential area were similar to those of the Korean population.25
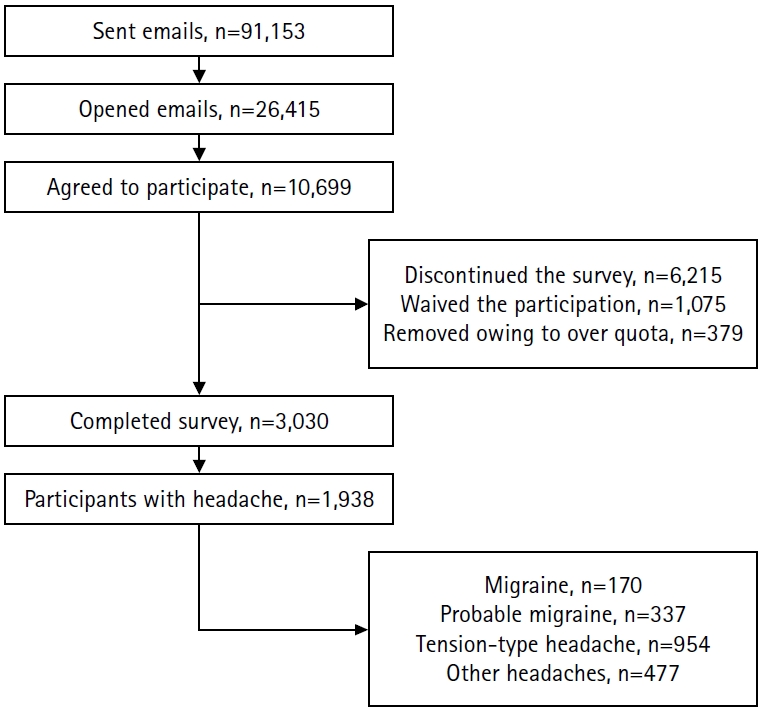
Recruitment of participants in the Circannual Change in Headache and Sleep (CHASE) study and diagnosis of headache.
Among the participants, 1,938 reported having a headache within the past year. The numbers meeting criteria for migraine, PM, TTH, and other headache diagnoses were 170, 337, 954, and 477, respectively. A total of 597 participants reported using rescue medication on more than 1 day in the past 30 days. There was no missing data because the survey required all fields to be completed.
2. Model selection and classification
Nine models, ranging from two to ten classes, were evaluated using LCA. Balancing statistical fit and classification quality with clinical interpretability, we selected the nine-class model because it best represented distinct class characteristics and had the lowest AIC and BIC, the LMR-LRT statistic, and the third-highest classification entropy (Table 1). The standard errors for the estimated class prior probabilities and the class-conditional response probabilities for the indicators were within acceptable ranges.
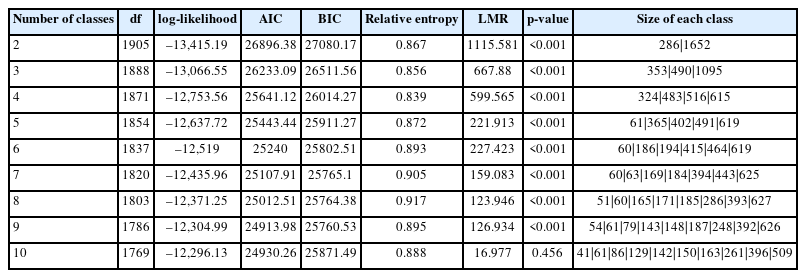
Model fit indices and class sizes for latent class analysis
3. Sociodemographic characters of the nine classes
Table 2 summarizes the sociodemographic features across the nine classes. There were no differences in education level or in comorbid hypertension, diabetes, or dyslipidemia. Class 1 was oldest group (41.78±10.89 years) and Class 8 was the youngest (37.93±10.62 years). However, this difference was not significant when multiple comparisons were made. Females comprised 56.1% of the overall headache cohort. However, Class 1 showed male predominance (54.2%) and differed significantly from Classes 4, 6, and 9, which showed female predominance (79.1%, 65.7%, and 62.0%, respectively). Class 4 had the strongest female predominance (79.1%) and differed significantly from Classes 3, 5, 7, and 9. Class 3 had a balanced sex distribution (50.4% male, 49.6% female). Body mass index (BMI) was significantly higher in Class 1 than in Class 4.
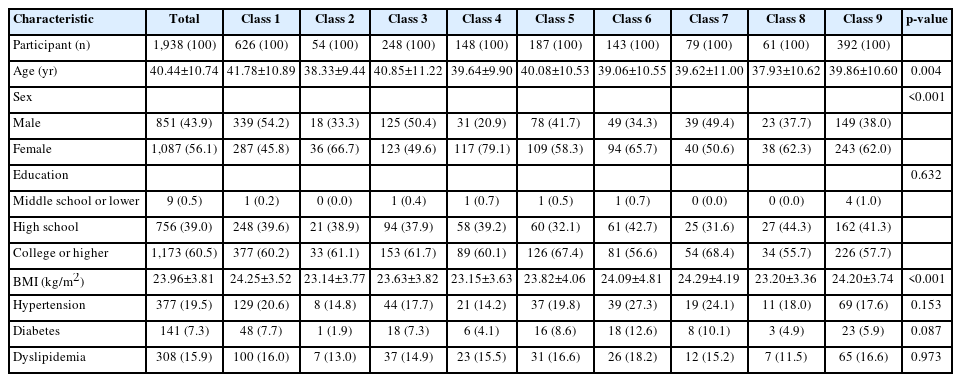
Sociodemographic features of the nine classes
4. Clinical features and associated characteristics of the nine classes
Headache characteristics and associated symptoms defined by the ICHD-3 criteria for migraine and TTH were used as variables in the LCA. Headache intensity, location, pulsating quality, aggravation by routine physical activity, nausea, vomiting, photophobia, phonophobia, headache frequency, and headache duration all differed significantly across classes (Table 3). Results of pairwise multiple comparisons are provided in the supplementary tables (Supplementary Table 2, available online).
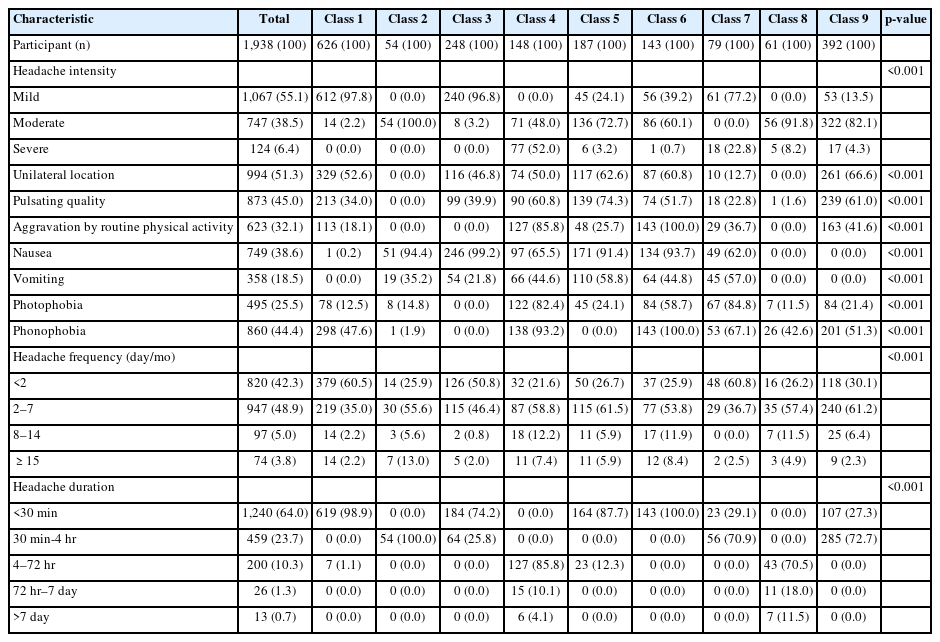
Differences in ICHD-3 diagnostic features across the nine latent classes
Other clinical characteristics, including headache-related impact, disability, comorbid symptoms, and the distribution of original ICHD-3 diagnoses across classes, are summarized in Table 4. The corresponding multiple comparisons are provided in the supplementary tables (Supplementary Table 3, available online).
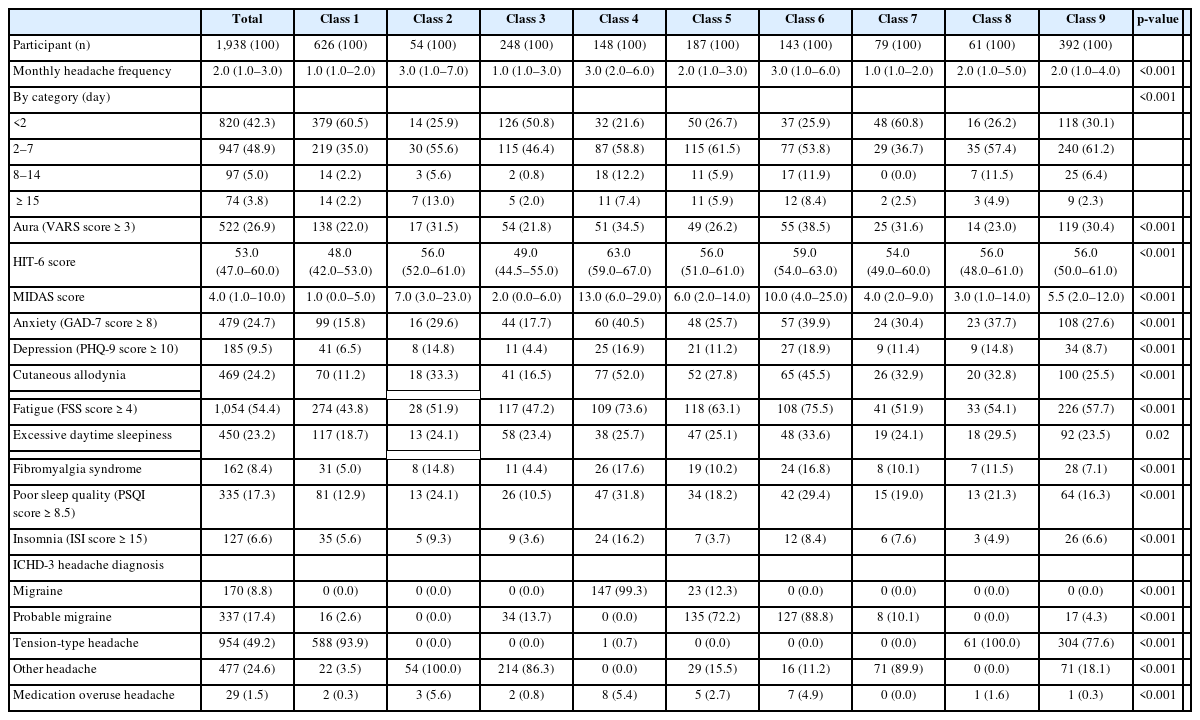
Comparison of clinical characteristics of the nine classes
Class 1 was the largest class, comprising 626 individuals (32.3%). Class 1 was characterized by mild headache intensity without nausea or vomiting, short duration (<30 minutes), and infrequent attacks (<8 day/mo). It also had the lowest HIT-6 and MIDAS scores and the lowest burden of anxiety, CA, fatigue, and EDS. 93.9% of Class 1 were TTH.
Class 2 (n=54) was characterized by uniformly moderate-intensity headache (100%) with nausea in 94.4%. Attacks lasted 30 minutes to 4 hours and were infrequent. Headache was predominantly bilateral, non-pulsatile, and not aggravated by routine physical activity. HIT-6 and MIDAS scores were moderately elevated. The presence of anxiety and depression was moderate across classes. The phenotype did not meet ICHD-3 criteria for migraine or TTH and all cases were classified as other headache disorder.
Class 3 (n=248) was characterized by mild headache intensity, nausea in 99.2%, absent photophobia and phonophobia, short duration (<4 hours), and infrequent attacks (<8 day/mo). Although this pattern resembles PM with short-duration, 86.3% were classified as other headache disorders, due to brief duration and mild headache intensity.
Class 4 (n=148) was characterized by moderate to severe headache intensity, unilateral location and pulsating quality in >50%, nausea and vomiting, and >80% of aggravation by routine physical activity, photophobia, and phonophobia. All attacks lasted ≥4 hours. Showing typical migraine features, 99.3% were migraine with one exception of TTH. Class 4 had the highest HIT-6 and MIDAS scores, the highest CA, anxiety, and FMS proportion. Depression presence was second highest.
Class 5 (n=187) was characterized by predominantly moderate-intensity headache with high proportion of unilateral location, pulsating quality, vomiting, and more nausea (91.4%). Photophobia was present in 24.1%, and phonophobia was absent. Attacks were generally infrequent (<8 day/mo) and of short duration. Of ICHD-3 headache diagnosis, 72.2% met criteria for PM and 12.3% for migraine.
Class 6 (n=143) was characterized by mild to moderate headache intensity with 100% aggravation by routine physical activity and 100% phonophobia. Photophobia occurred in 44.8%, and >50% had unilateral headache and pulsating quality. Attacks were brief (<30 minutes). Class 6 showed second-highest HIT-6, MIDAS, anxiety, FMS, and CA following Class 4. Class 6 showed the highest depression and visual aura. PM comprised 88.8% of this class.
Class 7 (n=79) was characterized by headache intensity that was either mild or severe (no moderate intensity), predominantly bilateral, non-pulsating, and with high rates of nausea, vomiting, photophobia (84.8%), and phonophobia. All attacks were short (<4 hours) and infrequent (<8 day/mo). Photophobia prevalence was the highest across classes. Visual aura was third highest, following Classes 6 and 4. In the original ICHD-3 diagnosis, 89.9% were other headache disorders.
Class 8 (n=61) was characterized by predominantly moderate to severe intensity, 100% bilateral location, and 98.4% non-pulsating quality, with no nausea, vomiting, or aggravation by routine physical activity. Photophobia occurred in 11.5% and phonophobia in 42.6%. Attacks lasted ≥4 hours. Headache impact, disability, and comorbidity burdens were moderate. All cases were classified as ICHD-3 TTH.
Class 9 (n=392) was the second-largest class, characterized by predominantly moderate-intensity headache, >60% unilateral and pulsating, no nausea or vomiting, photophobia in 21.4%, and phonophobia in 51.3%. Attacks were usually <4 hours. On ICHD-3 diagnosis, 77.6% were classified as TTH and 18.1% as other headache disorders.
DISCUSSION
The main findings were: 1) using ICHD-3 diagnostic features as variables, LCA identified nine headache classes; 2) class characteristics broadly mirrored established diagnostic categories (migraine, PM, TTH) while differing in severity, duration, and indices of sensory hypersensitization; 3) PM formed classes distinct from both migraine and TTH and showed a higher depression burden and more visual aura, supporting its clinical validity and the need for focused study; 4) several “other headache” classes were noted and showed meaningful burden with high proportion of photophobia or MOH, warranting clinical attention.
Diagnosing headache disorders is challenging.26 It relies on clinical criteria from the ICHD-3, with which many general practitioners are unfamiliar.27 Though there are proven pathophysiological differences between migraine, TTH, and cluster headache (CH), the ICHD-3 diagnostic criteria are defined by a combination of multiple variables, resulting in a variety of possible diagnoses.5 Furthermore, symptoms overlap between headache diagnoses, resulting in a grey zone, such as those with TTH and PM, whose final diagnosis is TTH.1,5,28 In other cases, a single headache diagnosis may present as multiple phenotypes, or multiple headache diagnosis may be made for a single patient.29,30 Consequently, a substantial proportion of patients are misdiagnosed and undertreated.26,31,32 Accurate diagnosis matters because migraine, TTH, and CH differ in their prognosis and their optimal treatment.33-35 Using a statistical approach, we examined overlap and potential misclassification in current criteria and identified natural diagnostic classes. Nine classes broadly mapped to ICHD-3 categories (Classes 1, 8, 9: TTH; Class 4: migraine; Classes 5, 6: PM; Classes 2, 3, 7: other headache) but differed in clinically relevant details. Whereas ICHD-3 primarily relies on frequency and duration to distinguish episodic from chronic phenotypes, our results indicate that severity and markers of central sensitization, specifically sensory hypersensitivities (photophobia, phonophobia) better differentiate classes. Photophobia, phonophobia, and CA have been associated with greater migraine severity and chronification.15,36 Our findings suggest these markers may be of more relevance than monthly frequency for classification of headache disorders.
Classes 1, 8, and 9 consisted mostly of TTH, but their characteristics differed. Together they comprised 1,079 participants (55.7%), slightly exceeding the number of TTH by ICHD-3 (n=954). Class 1 was male-predominant, had higher BMI, and was the most frequent. The profile reflects mild TTH (mild pain without nausea/vomiting), and the male predominance with a milder phenotype is consistent with prior epidemiologic studies.37 Class 9 was the second largest notable for >60% female, unilateral, and pulsating pain. However, most cases did not meet migraine or PM criteria because nausea or vomiting were absent, both photophobia and phonophobia were not present, and attacks were short (<4 hours). Only 17 individuals (4.3%) met PM criteria. Considered together, Classes 1 and 9, the two largest, were predominantly mild and more unilateral consistent with our prior report on unilateral TTH.2 Unilateral TTH warrants attention because it challenges the classical concept of TTH and may be misdiagnosed as migraine.2 Although both Class 1 and Class 9 reflected mild TTH, Class 9 showed greater headache impact, disability, depression, anxiety, and CA, indicating a mild but disabling phenotype that merits clinical attention. Differences between the two classes may reflect sex differences, as women tend to experience greater pain and disability than men, and treatment strategies should incorporate sex-specific considerations.38
In contrast, Class 8 showed classic bilateral headache without nausea or vomiting and had greater headache impact with poorer sleep indices, indicating the highest burden among TTH-like classes. Longer duration and more frequent attacks suggest a more severe, frequent or chronic TTH. Although relatively small, this subgroup may require more clinical care. The predominance of severe bilateral pain may have shaped the classic TTH concept, while milder phenotypes received less clinical attention. The high prevalence of TTH and variability emphasize the need for careful phenotyping and management, which remains under-recognized in clinical practice and research.2,34,37
Classes 2, 3, and 7 were predominantly other headaches (Class 2: 100%; Class 3: 86.3%; Class 7: 89.9%). Class 2 presented as a moderate-intensity other-headache phenotype. It had the highest attack frequency, with the largest proportion reporting ≥15 headache days per month. Headache was uniformly moderate, bilateral, non-pulsating, not aggravated by routine physical activity, and <4 hours in duration. The profile resembled TTH, but TTH was excluded because nausea was frequent (94.4%). Class 2 also had the highest prevalence of MOH (5.6%). In pairwise comparisons, MOH prevalence in Class 2 did not differ significantly from Class 4 (migraine) or Class 6 (PM with higher sensory sensitivity). Although much MOH literature focuses on migraine, TTH, and trigeminal autonomic cephalalgias such as CH, the MOH burden observed in this class warrants clinical attention given its potential for disability.39 Class 3 showed mild, short-duration headaches with frequent nausea (99.2%), without photophobia, phonophobia, or aggravation by routine physical activity. This class was predominantly other headache (86.3%), with only 13.7% meeting PM criteria. This class may represent a milder form of PM, positioned on the PM–migraine spectrum due to missing one or more diagnostic criteria. Because an “other headache” category in the current ICHD-3 can also present predominantly with nausea, more careful approach is recommended when using migraine screening tools that rely heavily on nausea.40,41 Class 7 was an “other headache” class with pronounced photophobia. It comprised short-duration headaches with the highest photophobia (84.8%) and the third highest phonophobia (67.1%), indicating prominent sensory hypersensitivity. However, CA was only the fourth most frequent across classes, and headache impact and disability were modest. This pattern likely reflects non-migraine phenotypes with heightened sensory sensitivity but without marked CA. Prior studies suggest that coexisting sensory hypersensitivities and CA are associated with greater disease burden than CA alone.42 The greater CA, depression, and headache impact in Class 6 relative to Class 7 may reflect these findings.
Class 4 displayed classic migraine features. ICHD-3 migraine comprised 99.3% (147/148) of individuals in this class and accounted for 86.5% (147/170) of all migraines in the study. Class 4 also had the highest burden across clinical scales (headache impact and disability) and the highest rates of CA, anxiety, fatigue, poor sleep quality, and insomnia. The proportion with MOH was second highest after Class 2. These findings support efficient ICHD-3 classification of the migraine phenotype in light of known pathophysiology.1,28 Migraine diagnoses outside Class 4 clustered mainly in Class 5 with PM, which showed a milder phenotype with fewer sensory hypersensitivities. Although migraine formed a distinct entity, several features commonly considered migraine-specific were not unique to Class 4. Unilateral pain was more frequent in Class 9 (predominantly TTH), pulsating quality in Class 5, and nausea was more prominent in Classes 3, 5, and 6. Prior population-based studies also report that up to 40% of individuals with migraine have bilateral pain.43 These observations indicate that the specificity of individual migraine symptoms warrants careful reappraisal given phenotypic heterogeneity and overlap.3,5
Classes 5 and 6 were predominantly PM. Both showed high nausea rates, moderate pain intensity, and frequent unilateral location. Headache duration was <30 minutes in all of Class 6 and in most of Class 5, consistent with prior Korean data in which short duration was the most common reason for PM diagnosis.8 Regional epidemiology should be considered, as lower migraine prevalence and higher PM rates have been reported in Korean, African American populations compared with white populations.8,32 The concentration of PM in these two classes suggests that PM, often not coded when a more definitive diagnosis is assigned, warrants greater diagnostic attention as a distinct phenotype within the migraine spectrum. The classes differed in that Class 6 had 100% aggravation by routine physical activity and 100% phonophobia, whereas phonophobia was absent in Class 5. Class 5 represents a comparatively milder PM profile without phonophobia. Class 6 represents PM with prominent sensory hypersensitivity. Class 6 showed a higher burden. It had second-highest HIT-6, MIDAS, and CA after Class 4, and the highest proportion of visual aura, depression, fatigue, and EDS. It is important to note that the burden in class 6 exceeded that in class 4, migraine. The finding stresses the need for targeted assessment and management of PM, which remains undertreated.32
Photophobia, phonophobia, and CA, hallmarks of central sensitization, were among the most discriminative features separating classes with similar ICHD-3 diagnosis (e.g., 5 vs. 6 and 7 vs. 2 or 3). Sensory hypersensitivities and CA are clinical correlates of central sensitization and are associated with greater migraine burden and a higher risk of progression to chronic migraine.36,44 Co-existence of multiple hypersensitivities (photophobia, phonophobia, osmophobia) and CA correlates with more severe migraine, through central sensitization and nociceptive pathway alteration.36,42 While ICHD-3 distinguishes episodic and chronic forms by monthly headache days, our findings suggest that features of central sensitization may reflect disease severity.1
While ICHD-3 migraine diagnosis requires photophobia and phonophobia for a diagnostic criterion,1 in our data, photophobia and phonophobia contributed differently to class separation, which may reflect distinct pathophysiology. Photophobia has been linked to a retino–thalamo–cortical pathway, whereas phonophobia has been associated with auditory neurons and brainstem auditory systems.45,46 Recognizing possible pathophysiologic heterogeneity, additional research is required for development of more precise diagnostic criteria.
Our study has several limitations. First, headache diagnoses relied on patient self-report, which may introduce bias. Recall of headache characteristics and frequency may have been influenced, and duration may have been affected by medication use. However, we queried duration as if rescue medication had not been taken, and the diagnostic algorithm has been validated with acceptable sensitivity and specificity.12 Second, because the survey queried only each participant’s most severe headache, overlapping or concurrent diagnoses were not captured. However, diagnosing multiple headaches is difficult without a headache diary,30 particularly in a population-based study. Third, the questionnaire was designed to diagnose migraine, PM, and TTH and was not intended to diagnose other primary headaches or post-traumatic headache, so some “other headache” cases could include TACs such as CH. However, the predominantly bilateral pattern, mild to moderate severity distribution, and the low population prevalence of TACs make substantial inclusion unlikely. Fourth, although nationwide, the sample comprised only Korean adults, so generalizability to other populations is uncertain given racial differences in migraine and PM prevalence,32 and replication in more diverse cohorts is warranted. In addition, although local independence is a fundamental assumption of LCA, post-estimation checks using bivariate residuals indicated only limited residual associations. These were primarily observed among clinically related symptom pairs and did not meaningfully alter the emergent class structure. Lastly, the statistically derived classes were interpreted clinically but do not by themselves establish distinct pathophysiology. Further studies are needed to confirm the proposed classification.
Conclusions
In this population-based study, we identified natural classes of headache by LCA of ICHD-3 diagnostic features. Nine clinically distinct classes emerged whose core characteristics paralleled migraine, PM, TTH, and other headaches, while differing in severity, duration, and markers of sensory hypersensitization. One migraine and three TTH phenotypes were noted. PM formed discrete classes separable from both migraine and TTH. One of the two PM classes with exclusive phonophobia had the highest depression burden, and one of the three “other headache” classes carried a high MOH burden, drawing clinical attention. These findings challenge current diagnostic frameworks and motivate studies to refine diagnostic classification with pathophysiologic evidence.
Notes
AVAILABILITY OF DATA AND MATERIAL
The data presented in this study are available upon reasonable request from the corresponding author.
AUTHOR CONTRIBUTIONS
Conceptualization: WL, MKC; Data curation: WL, SJH, JY, MKC; Formal analysis: WL, SJH, MKC; Investigation: WL, JY, MKC; Methodology: WL, SJH; Writing–original draft: WL, SJH; Writing–review & editing: WL, SJH, JY, MKC.
CONFLICT OF INTEREST
Seok-Jae Heo and Jungyon Yum declare no conflicts of interest. Wonwoo Lee was involved as a site investigator in a multicenter trial sponsored by Eli Lilly and Co., WhanIn Pharm Co. Ltd., and Handok-Teva. He has received lecture honoraria from Abbott and SK chemical in the past 24 months. Min Kyung Chu was a site investigator for a multicenter trial sponsored by Allergan Korea, Biohaven Pharmaceuticals, and Lundbeck Korea. He has received lecture honoraria from Allergan Korea, Handok-Teva, Eli Lilly and Company, and Yuyu Pharmaceutical Company in the past 24 months. Additionally, he received grants from Yonsei University College of Medicine (6-2021-0229), the Korea Health Industry Development Institute (KHIDI) (HV22C0106), and National Research Foundation of Korea (2022R1A2C1091767).
FUNDING STATEMENT
This study was supported by a 2023 research grant for the headache research group, from the Headache Research Committee of the Korean Headache Society.
ACKNOWLEDGMENTS
Grammatical revisions were supported by ChatGPT (versions 4o–5.2).
SUPPLEMENTARY MATERIAL
Supplementary materials are available from https://doi.org/10.62087/hpr.2026.0004.
Bivariate residuals assessing local independence among observed indicators in the latent class analysis
Supplementary Table for pairwise comparison of features in Table 3
Supplementary Table for pairwise comparison of features in Table 4