Temporal Evolution and Multimodal Neuroimaging in Reversible Cerebral Vasoconstriction Syndrome, Arterial Dissection, and Cerebral Venous Thrombosis
Article information

Abstract
Cerebrovascular disorders are important secondary causes of headache, but diagnosis can be challenging because headache may be the earliest or only presenting symptom and initial neuroimaging findings are often normal or nonspecific. This review provides a systematic, imaging-focused discussion of three representative cerebrovascular headache disorders: reversible cerebral vasoconstriction syndrome (RCVS), cervical and intracranial artery dissection, and cerebral venous thrombosis (CVT). For each condition, we describe characteristic findings across relevant imaging modalities, including computed tomography, computed tomography angiography, magnetic resonance imaging (MRI), magnetic resonance angiography, vessel wall (VW)-MRI, and susceptibility-sensitive sequences. We also discuss the temporal evolution of imaging findings, which underlies several common diagnostic pitfalls. In RCVS, angiographic vasoconstriction propagates centripetally from distal to proximal vessels, and contrast-enhanced fluid-attenuated inversion recovery imaging can detect blood–brain barrier disruption before vasoconstriction becomes angiographically apparent. In arterial dissection, VW-MRI can show mural features that confirm the diagnosis and may help stratify ischemic risk. In CVT, susceptibility-weighted imaging improves detection of cortical vein thrombosis, a subtype that can be missed on conventional venography. Across all three conditions, single-time-point imaging may be misleading, and serial imaging is often needed to increase diagnostic certainty because interval changes may reveal findings not present on the initial study. By integrating modality-specific findings with their temporal dynamics, this review proposes a practical imaging framework for the early and accurate diagnosis of cerebrovascular secondary headache disorders.
INTRODUCTION
Headache is one of the most common neurological symptoms encountered in clinical practice and a leading cause of disability worldwide. The Global Burden of Disease Study 2023 estimates that 2.9 billion individuals are affected globally, ranking sixth among all causes of years lived with disability and underscoring its substantial public health impact.1,2 While most cases are attributable to primary headache disorders without structural abnormalities, a clinically important subset arises secondary to identifiable underlying conditions. The International Classification of Headache Disorders, third edition, recognizes a broad spectrum of secondary headache diagnoses, reflecting this diagnostic breadth.3 In this context, the key clinical challenge lies not in diagnosing primary headache, but in identifying patients in whom headache signals a potentially serious and treatable underlying pathology. Structured approaches, such as the SNNOOP10 framework, provide practical guidance for recognizing these warning presentations and selecting patients who require urgent neuroimaging.4
Among secondary headache disorders, cerebrovascular etiologies deserve particular attention because headache may be the earliest—and sometimes the sole—clinical manifestation, preceding focal neurological deficits by hours to weeks.5 Reversible cerebral vasoconstriction syndrome (RCVS), cervical and intracranial artery dissection, and cerebral venous thrombosis (CVT) are three conditions that exemplify this pattern. RCVS reflects reversible dysregulation of cerebral arterial tone, arterial dissection involves intramural hematoma from arterial wall injury, and CVT arises from venous occlusion with consequent venous hypertension. Despite these mechanistic differences, all three can present with isolated headache, including thunderclap onset, before any additional neurological signs develop.5-9 These disorders also share a critical diagnostic challenge: neuroimaging findings may be absent or inconclusive at initial presentation, and their radiologic features evolve dynamically over time. In RCVS, angiographic vasoconstriction may be delayed for up to 2 weeks after headache onset.6,7 In arterial dissection, intramural hematoma can appear isointense on early T1-weighted imaging, producing a false-negative result.10 In CVT, acute thrombus signal on conventional magnetic resonance imaging (MRI) may mimic a normal flow void.11 The combination of clinical urgency, early imaging ambiguity, and temporal evolution makes these three entities particularly instructive to examine together from an imaging perspective.
This review examines the multimodal neuroimaging findings of RCVS, arterial dissection, and CVT, with particular emphasis on temporal evolution, follow-up imaging, and the practical imaging clues that help distinguish these disorders from common mimics.
REVERSIBLE CEREBRAL VASOCONSTRICTION SYNDROME
RCVS is defined by acute severe headache, typically thunderclap headache (TCH), together with multifocal narrowing of the cerebral arteries that typically resolves within 3 months of onset.7,12 Although this reversibility criterion remains central to the current diagnostic framework, delayed or incomplete resolution beyond 3 months has been reported in a subset of patients,13,14 and recurrent episodes can occur after intervals of months to years.15,16 The syndrome encompasses several previously described entities—including Call-Fleming syndrome, benign angiopathy of the central nervous system, postpartum angiopathy, and drug-induced angiopathy—unified under standardized diagnostic criteria proposed by Calabrese et al.12 in 2007. RCVS predominantly affects women in mid-adult life, with a population incidence estimated at approximately 2.7 cases per million annually, though this likely underestimates the true burden given the potential for early false-negative vascular imaging.17-20
TCH reaching maximal intensity within 1 minute is the clinical hallmark. Attacks are typically recurrent over several days and are frequently provoked by exertion, sexual activity, Valsalva maneuver, emotion, or water contact.6,7,17 Atypical presentations with gradual-onset or absent headache account for up to 15% of cases.21 Secondary causes include postpartum state, vasoactive drugs (serotonergic agents, triptans, ergot derivatives), illicit substances, and catecholamine-secreting tumors, though the proportion varies widely across cohorts.17,19 The REVERCE network (1,127 patients across Europe and Asia) documented substantially higher rates of secondary triggers, brain lesions, and worse outcomes in European compared to Asian patients.22
1. Cerebral angiography and non-invasive vascular imaging
Catheter digital subtraction angiography (DSA) has historically served as the reference standard for detecting the characteristic “string of beads” pattern—alternating segments of stenosis and normal or dilated arterial caliber in multiple cerebral arteries.7,12 In a large RCVS–primary angiitis of the central nervous system (PACNS) comparative series (n=159 RCVS), this pattern was observed in 68% of patients, with symmetric bilateral involvement in 82%.23 Medium-caliber arteries, predominantly M2/M3 middle cerebral artery (MCA) and posterior cerebral artery (PCA) branches, are most commonly affected (Figure 1).7,24
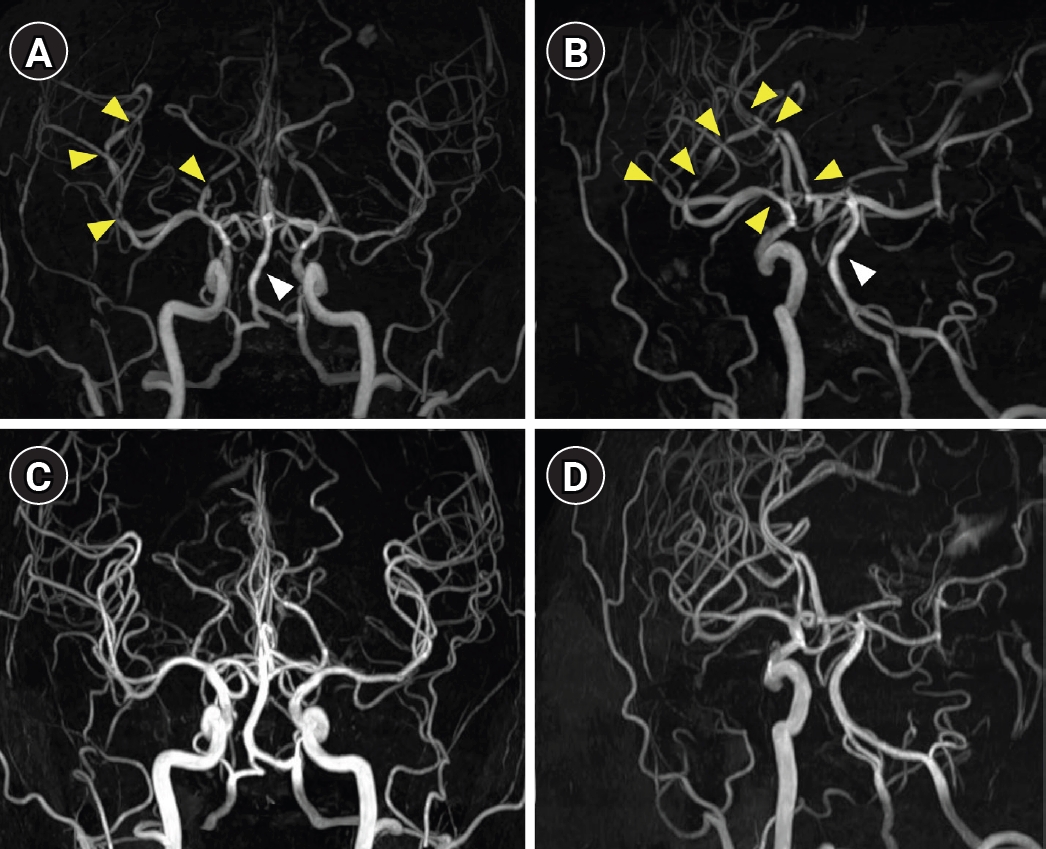
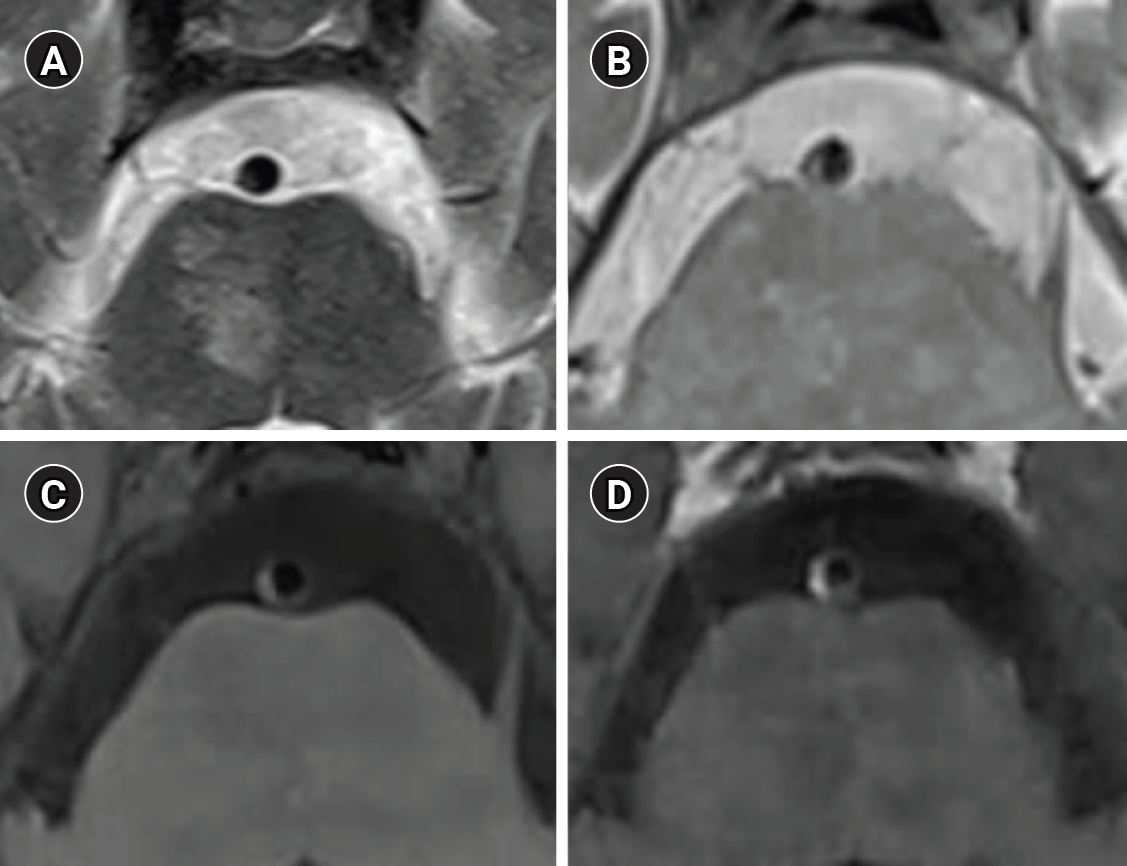
Typical reversible cerebral vasoconstriction syndrome (RCVS) on serial magnetic resonance angiography (MRA). (A, B) Initial MRA demonstrates the classic “string-of-beads” pattern, with multifocal alternating segments of stenosis and dilatation involving the middle cerebral artery, anterior cerebral artery, and posterior cerebral artery branches (yellow arrowheads), with additional irregularity of the basilar artery (white arrowheads). Arrowheads indicate selected representative lesions in clearly visible locations; additional focal vasoconstrictions are present in other intracranial arteries. (C, D) Follow-up MRA at 3 months demonstrates complete resolution of the vascular abnormalities in this representative case, supporting the diagnosis of RCVS.
Computed tomography angiography (CTA) and magnetic resonance angiography (MRA) are both appropriate first-line studies, with approximately 80% sensitivity relative to DSA.25 MRA is often preferred as the initial modality because it avoids radiation and iodinated contrast exposure. It also offers standardized imaging parameters that enhance reproducibility and can be combined with brain MRI and complementary sequences such as susceptibility-weighted imaging (SWI), vessel wall (VW) imaging, and contrast-enhanced fluid-attenuated inversion recovery (CE-FLAIR) in a single session.24,26 CTA, however, provides more accurate anatomical depiction of vessel morphology and is less susceptible to flow-related artifacts, making it particularly useful when rapid assessment is needed or when MRA findings are equivocal (Figure 2).24,27 A critical pitfall shared by both modalities is early false-negative imaging: in the French prospective cohort, 21% of patients had a normal initial MRA despite ultimately proven RCVS.17 Peak vasoconstriction is reached approximately 16 days after symptom onset,7,26 and transcranial Doppler demonstrates elevated MCA velocities in approximately 69% of patients during active disease.17,24 When clinical suspicion is high based on recurrent triggered TCH, repeat vascular imaging at 1–2 weeks is essential even when the initial study is unremarkable. DSA is currently reserved for cases in which noninvasive imaging remains inconclusive or the patient clinically deteriorates, although it carries a risk of procedure-related clinical worsening.28
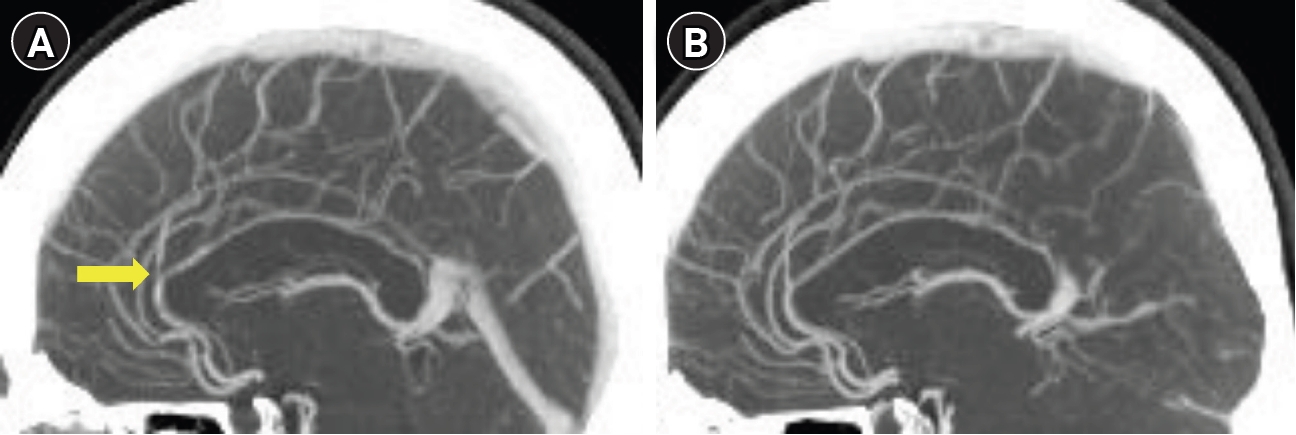
Reversible cerebral vasoconstriction syndrome (RCVS) on computed tomography angiography (CTA) with multiplanar reformatted images. (A) Initial CTA demonstrates multifocal alternating stenosis and dilatation, with prominent involvement of the anterior cerebral artery (yellow arrow). Depending on the case, multiplanar reformatted images may help assess the extent of arterial involvement. (B) Follow-up CTA at 3 months demonstrates complete resolution of the vascular abnormalities in this case, consistent with RCVS.
Beyond the classic multifocal beaded pattern, the angiographic spectrum of RCVS includes atypical presentations—such as single-segment stenosis, focal dilatation, or diffuse smooth narrowing—that may mimic intracranial atherosclerosis or dissection (Figure 3).29 Time-of-flight (TOF)-MRA is additionally susceptible to flow-related artifacts that can produce pseudo-stenosis, further complicating interpretation.29 Serial imaging correlated with the clinical timeline, rather than reliance on a single examination, is therefore integral to the diagnosis.
Reversible cerebral vasoconstriction syndrome (RCVS) mimicking intracranial atherosclerosis. (A) Initial computed tomography angiography (CTA) demonstrates long-segment stenosis of the distal middle cerebral artery (arrow). The posterior cerebral artery segment (arrowhead) also shows subtle alternating dilatation, which is more suggestive of RCVS. The arrow and arrowhead indicate selected representative findings. (B) Follow-up CTA at 3 months demonstrates complete resolution of the vascular abnormalities in this case, clarifying the diagnosis as RCVS rather than intracranial atherosclerosis.
2. Brain magnetic resonance imaging
Brain MRI is normal in a substantial proportion of patients during the first days; when abnormal, it typically shows one or more of the following patterns.
Acute ischemic infarction on diffusion-weighted imaging (DWI) characteristically follows a bilateral cortical-subcortical border zone (watershed) distribution, reflecting hemodynamic compromise from upstream vasoconstriction; in the RCVS–PACNS comparison, 88% of ischemic strokes in RCVS followed this pattern, yielding a positive predictive value of 97% for distinguishing RCVS from PACNS.7,23 Conversely, deep gray matter or brainstem infarcts are characteristic of PACNS.23 The FLAIR hyperintense vessel sign, reflecting sluggish flow distal to vasoconstricted segments, may be seen in a subset of patients and has diagnostic utility for distinguishing RCVS from PACNS.23
SWI or gradient-echo (GRE) sequences should always be reviewed to detect convexal subarachnoid hemorrhage (cSAH) and small lobar hemorrhages, which may be subtle on routine sequences.30,31 Posterior reversible encephalopathy syndrome (PRES)-like vasogenic edema, when present, manifests as bilateral, symmetric FLAIR hyperintensity in the parieto-occipital regions.32 The prevalence, timing, and clinical significance of ischemic infarction, hemorrhagic complications, and PRES are detailed in the Complications subsection below.
3. Vessel wall magnetic resonance imaging
Intracranial VW-MRI is most useful when luminal imaging is equivocal or when the primary differential diagnosis includes PACNS, intracranial atherosclerotic disease (ICAD), or dissection.33 According to the American Society of Neuroradiology (ASNR) consensus recommendations, 3T black-blood protocols with isotropic voxel dimensions of 0.4–0.7 mm and pre- and post-contrast T1-weighted, T2-weighted, and TOF-MRA sequences are recommended.33
The characteristic finding in RCVS is diffuse circumferential wall thickening with absent or minimal gadolinium enhancement, reflecting smooth muscle contraction without significant inflammatory infiltration.13 In the series by Obusez et al.13 comparing 13 RCVS and 13 central nervous system vasculitis patients, 77% of RCVS patients showed diffuse uniform thickening with negligible-to-mild enhancement, and all patients with follow-up imaging demonstrated complete resolution, although notably this required up to 3.5 months in some cases, exceeding the conventionally cited 3-month window. A subsequent prospective 3T study by Chen et al.14 found enhancement in 45.8% of patients, predominantly mild (77%) and concentric (73%), with incomplete resolution at follow-up in 36%. The key discriminator is therefore not the mere presence or absence of enhancement, but rather the combination of enhancement pattern and its temporal evolution: in RCVS, mild concentric wall enhancement may appear in the early phase and usually resolves on follow-up imaging, most often within approximately 3 months, although incomplete resolution has been reported in up to 36% of patients on follow-up VW-MRI.14 By contrast, PACNS demonstrates strong, persistent wall enhancement that may persist over months to years (Table 1). Accordingly, persistent vascular abnormalities beyond 3 months should prompt careful reassessment for alternative arteriopathies, but should not automatically exclude RCVS when the overall clinical presentation and temporal imaging evolution remain compatible.
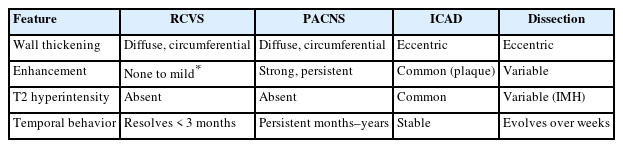
Vessel wall MRI discriminators in intracranial vasculopathies
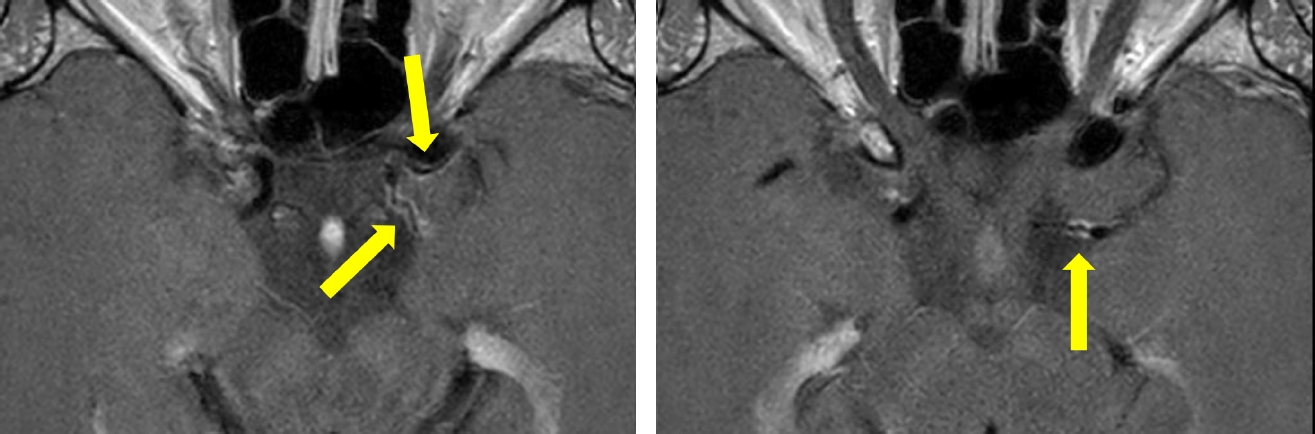
The temporal dimension of this distinction is further reflected in Table 2, which summarizes the broader role of serial imaging in confirming reversibility in RCVS and distinguishing it from fixed or inflammatory arteriopathies. PACNS shows strong persistent enhancement (100%) with no T2 hyperintensity (Figure 4).13,33,34 ICAD demonstrates eccentric wall thickening with T2 hyperintensity (79% sensitivity, 100% specificity versus RCVS and vasculitis combined), and the combination of eccentric morphology with T2 signal achieves 96.3% sensitivity for ICAD (Figure 5).34 Dissection is identified by an intimal flap or evolving intramural T1 hyperintensity reflecting methemoglobin formation.33
Temporal evolution and role of serial imaging in RCVS, arterial dissection, and CVT
Vessel wall magnetic resonance imaging findings in primary angiitis of the central nervous system. Persistent wall enhancement remains evident on follow-up imaging 2 months after symptom onset, in contrast to the minimal or resolving enhancement typically seen in reversible cerebral vasoconstriction syndrome (yellow arrows).
Vessel wall magnetic resonance imaging of basilar artery atherosclerosis with pontine infarction due to branch artery occlusion. (A) T2-weighted image. (B) Proton density-weighted image demonstrates eccentric wall thickening. (C) Pre-contrast and (D) post-contrast T1-weighted images show mild eccentric enhancement of the thickened wall, compatible with an atherosclerotic plaque.
4. Temporal evolution and centripetal propagation
A distinctive feature of RCVS is the centripetal propagation of vasoconstriction from distal to proximal vessels over time. Initial vasoconstriction begins in small peripheral cortical arteries below the resolution of non-invasive imaging and spreads toward larger proximal vessels over days (Figure 6).7,24 Shimoda et al.35 documented this directly in 16 patients imaged within 72 hours and again at TCH resolution (mean 8.5 days): propagation to M1 MCA (62.5%), P1 PCA (62.5%), and A1 anterior cerebral artery (31.3%) was observed in 87.5% of patients, and 15 of 16 patients showed persistent or worsening vasoconstriction even after headache remission.
Centripetal propagation of reversible cerebral vasoconstriction syndrome (RCVS) on serial magnetic resonance angiography (MRA). (A) MRA obtained on day 4 after headache onset shows segmental stenoses confined to distal branches of the anterior, middle, and posterior cerebral arteries (yellow arrows). (B) Follow-up MRA on day 19 demonstrates extension of vasoconstriction to more proximal arterial segments, including the basilar artery, with more prominent stenosis and dilatation (yellow arrowheads). This serial pattern illustrates the characteristic centripetal progression of RCVS and supports repeat imaging when initial findings are subtle.
This pattern accounts for two paradoxes frequently encountered in clinical practice: early CTA or MRA may be entirely normal because vasoconstriction remains confined to distal vessels below imaging resolution, and headache may improve while proximal-vessel vasoconstriction is actually progressing on follow-up angiography. In a longitudinal study of 186 patients, angiographic vasoconstriction severity peaked during the third week, approximately 1 week after peak blood–brain barrier (BBB) breakdown.36 These findings underscore that symptom resolution is not a reliable endpoint for imaging surveillance. Although the 3-month reversibility criterion remains a useful diagnostic benchmark, not all patients conform strictly to this time frame. Delayed or incomplete resolution of vascular abnormalities has been documented on follow-up imaging,13,14 and long-term cohort studies have shown that recurrent RCVS can occur after intervals of months to years.15,16 These observations support interpreting the 3-month criterion as a practical diagnostic framework rather than an absolute boundary.
5. Blood–brain barrier breakdown on magnetic resonance imaging
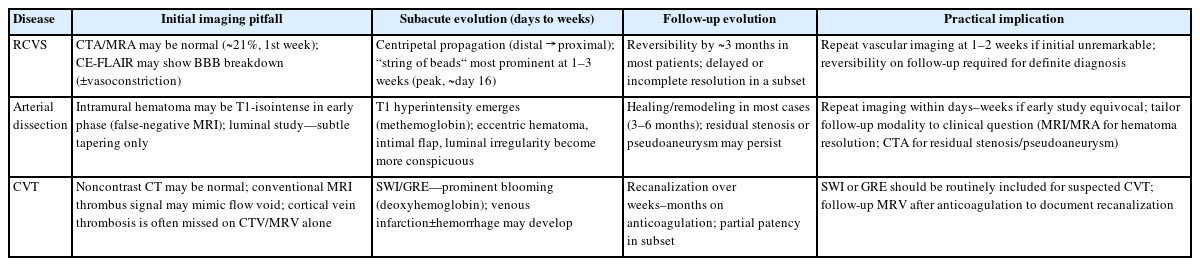
CE-FLAIR is currently one of the most informative MRI markers of BBB dysfunction in RCVS. Lee et al.37 detected BBB breakdown by CE-FLAIR in 69% of definite RCVS patients, with multifocal sulcal and leptomeningeal enhancement predominantly over the convexities and falx (Figure 7). BBB breakdown was independently associated with neurological complications.37 Beyond prognostic implications, CE-FLAIR positivity can support the diagnosis of probable RCVS in patients with typical TCH but initially normal angiography, raising the diagnostic yield beyond luminal imaging alone.29,37
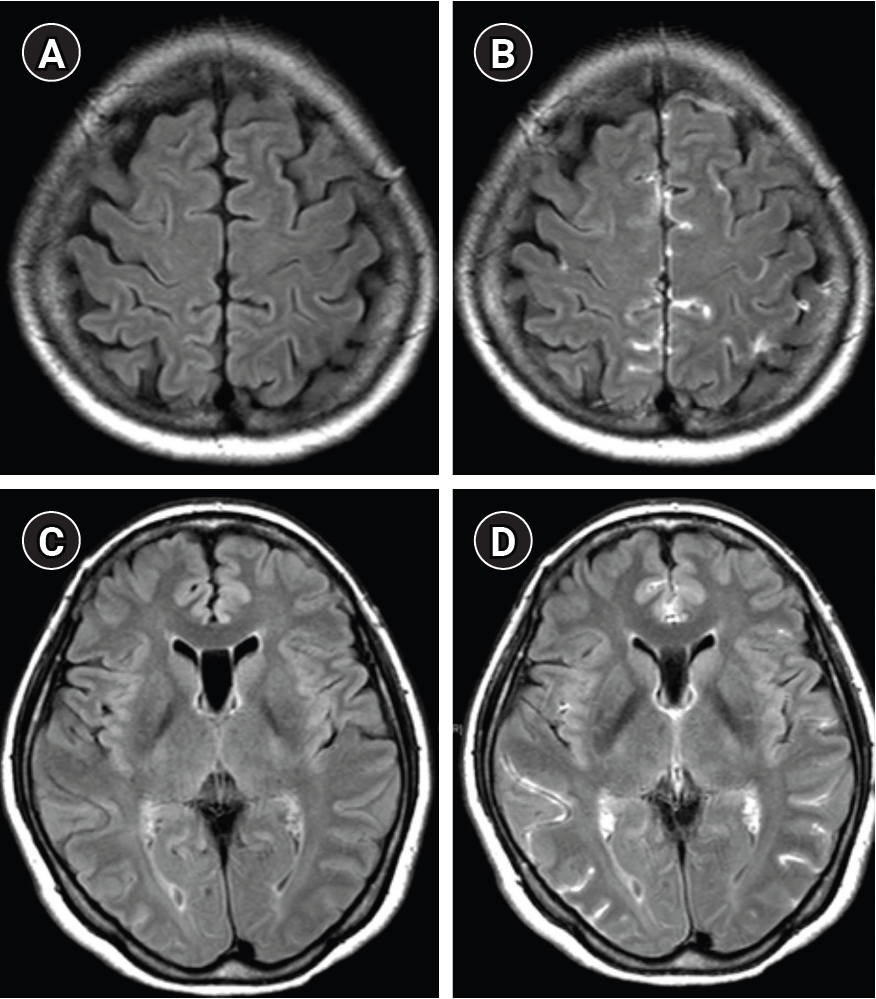
Blood–brain barrier (BBB) disruption detected by contrast-enhanced fluid-attenuated inversion recovery (FLAIR) imaging in reversible cerebral vasoconstriction syndrome. (A, C) Non-contrast FLAIR images show no definite subarachnoid signal abnormality. (B, D) Corresponding contrast-enhanced FLAIR images demonstrate hyperintense cerebrospinal fluid signal, indicating BBB disruption. Modified from the article of Kim et al. (J Headache Pain 2025;26:89).29
Temporally, BBB breakdown peaks during the second week (56.8% prevalence), whereas angiographic vasoconstriction peaks in the third week.36 Blood pressure surge was the strongest independent predictor of BBB breakdown extent, with a synergistic interaction with early imaging timing.36 This temporal dissociation supports BBB dysfunction as an early pathophysiological event that precedes—rather than merely follows—the period of maximal hemodynamic compromise.
6. Diagnostic approach when vessel wall magnetic resonance imaging is unavailable
Access to high-resolution VW-MRI remains limited in many clinical settings. In such circumstances, a structured approach combining serial noninvasive vascular imaging, CE-FLAIR, and clinical scoring systems can support the diagnosis without VW-MRI. The cornerstone is repeat CTA or MRA at 1–2 weeks when the initial study is unremarkable, as outlined in Table 2; this strategy directly addresses the centripetal propagation pattern and the second- to third-week peak of vasoconstriction that characterize RCVS. CE-FLAIR can support the diagnosis even when initial angiography is normal, by demonstrating sulcal hyperintensity consistent with BBB breakdown.37 On parenchymal MRI, a bilateral cortical-subcortical border-zone pattern of acute infarction on DWI is highly characteristic of RCVS, with a positive predictive value of 97% in distinguishing RCVS from PACNS,23 and, once aneurysmal subarachnoid hemorrhage (aSAH) has been excluded, an isolated cSAH in this clinical context further supports the diagnosis.31 Clinical scoring systems complement imaging: the RCVS2 score helps distinguish RCVS from other intracranial arteriopathies when vascular imaging is abnormal, and the RCVS-TCH score identifies RCVS among patients with TCH, even before angiographic confirmation.38,39
7. Complications
Hemorrhagic complications develop within the first week in 34%–43% of patients.17,30 cSAH is the most frequent (22%–38%), restricted to cortical sulci (Figure 8).31 Intraparenchymal hemorrhage occurs in 6%–13%, predominantly as small lobar hematomas; risk factors include female sex, older age, and migraine history.30,31
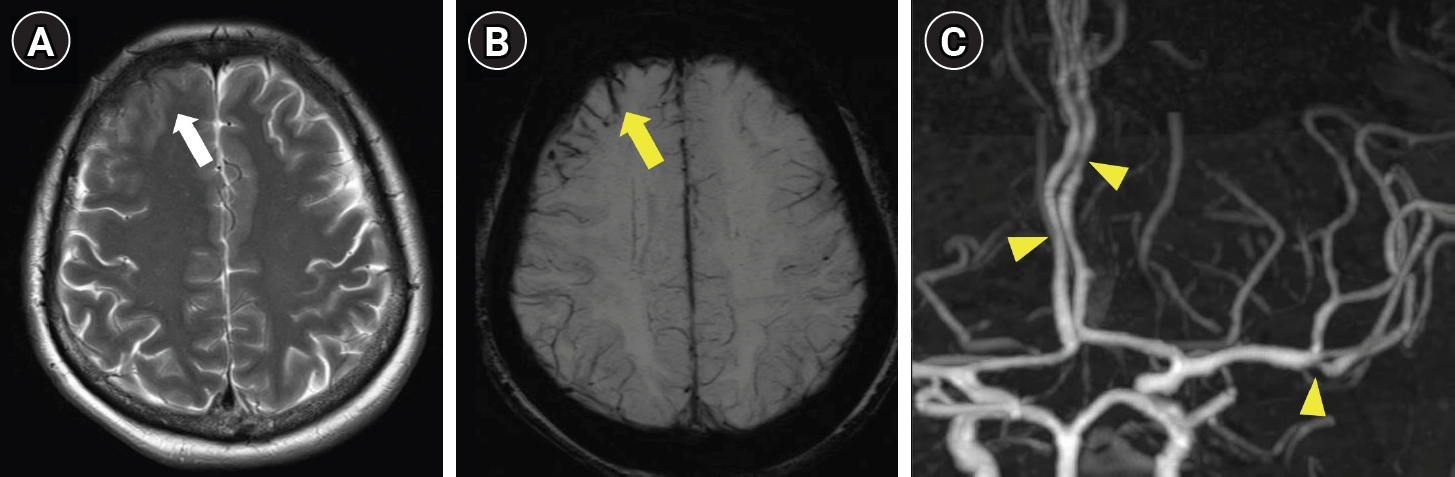
Cortical edema and convexal subarachnoid hemorrhage in reversible cerebral vasoconstriction syndrome. (A) T2-weighted image demonstrates cortical edema in the right frontal lobe (white arrow). (B) Susceptibility-weighted image shows minimal convexal subarachnoid hemorrhage overlying the affected cortex (yellow arrow). (C) Magnetic resonance angiography demonstrates multifocal stenosis of the cerebral arteries (yellow arrowheads).
Ischemic stroke develops in approximately 6%–39% of patients, characteristically in the second to third week, after the hemorrhagic peak;7,23,30 angiographic severity predicts ischemic stroke risk.30 When the border-zone infarct pattern is combined with recurrent TCH, the composite carries a 100% positive predictive value for RCVS over PACNS.23
PRES-like vasogenic edema is a recognized complication, occurring in 9% of patients in early prospective series17 and 25%–28% in later angiogram-based cohorts,23,24 typically within the first 1–2 weeks. In this context, PRES is best understood as an overlapping complication within the RCVS spectrum—sharing upstream mechanisms of BBB dysfunction and blood pressure surge—rather than a separate imaging entity.32 Clinical worsening after initial diagnosis occurs in 34% of patients at a median of 2.5 days, resulting in permanent neurological deficit in 40% of those who worsen.28 Conventional angiography was associated with clinical deterioration in 14% of patients within 24 hours of the procedure, supporting the preferential use of noninvasive imaging during the unstable phase.28
8. Differentiation from aneurysmal subarachnoid hemorrhage
aSAH is the most important real-world differential diagnosis for RCVS presenting with TCH, and the two can occasionally coexist because small convexal hemorrhage is itself a recognized complication of RCVS.31 Hemorrhage distribution provides the principal imaging discriminator: aSAH produces basal cisternal blood centered on the circle of Willis, whereas RCVS-related hemorrhage is restricted to cortical sulci of the convexity.31 In the emergency department, a stepwise approach to TCH is consistent with current acute-headache guidelines.40,41 Noncontrast computed tomography (CT) within 6 hours of headache onset has very high sensitivity for aSAH and is the appropriate first study;42 sensitivity declines beyond 6 hours, requiring CTA or lumbar puncture as the next step. Lumbar puncture confirms aSAH through xanthochromia and red blood cells, whereas cerebrospinal fluid (CSF) is typically normal or near-normal in RCVS.12 CTA can simultaneously assess luminal findings across multiple cerebrovascular causes of TCH—vasoconstriction in RCVS, tapering or pseudoaneurysm in dissection, and, when the protocol is extended to include computed tomography venography (CTV), venous filling defects—although mural hematoma in dissection is best characterized on MRI. As an adjunctive sequence, CE-FLAIR can support an RCVS diagnosis by demonstrating sulcal hyperintensity from BBB breakdown that frequently precedes angiographic changes.36
CERVICAL AND INTRACRANIAL ARTERY DISSECTION
Cervical and intracranial artery dissection is a major cause of ischemic stroke in young and middle-aged adults and represents a prototypical arteriopathy in which structural disruption of the VW leads to characteristic imaging findings. This process, typically initiated by an intimal tear and/or hemorrhage into the VW, results in intramural hematoma, luminal stenosis or occlusion, and occasionally pseudoaneurysmal dilatation.10,43 Cervical artery dissection is an important cause of ischemic stroke in young and middle-aged adults, with reported annual incidence ranging from 2.6 to 4.7 per 100,000 persons and accounting for up to 25% of strokes in adults under 50 years.43-45 Most cases involve the extracranial internal carotid or vertebral artery, whereas intracranial artery dissection is less common but deserves special attention because it may present with subarachnoid hemorrhage, ischemic stroke, or brainstem mass effect.43,46 Intracranial artery dissection has a distinct clinical profile: it predominantly involves the V4 segment of the vertebral artery, affects patients at a somewhat older mean age, carries a 50%–60% risk of subarachnoid hemorrhage, and shows a notable predilection for East Asian populations.8,46 From the headache perspective, dissection is a high-yield example of a stroke syndrome in which local pain frequently precedes or dominates the early presentation.5
Headache and neck pain are the most common initial manifestations and frequently precede neurological deficits by hours to weeks.8,43 Internal carotid artery dissection typically produces ipsilateral frontotemporal or periorbital pain, often accompanied by partial Horner syndrome; vertebral artery dissection (VAD) more often causes posterior neck pain or occipital headache and may be associated with posterior circulation ischemia.8,43,47 Thunderclap onset occurs in approximately 20% of pain-dominant presentations, requiring urgent differentiation from aneurysmal subarachnoid hemorrhage and RCVS.47 Importantly, pain may be the sole manifestation in up to 34% of cases, most notably in extracranial VAD, and the interval from headache onset to ischemic stroke can range from minutes to several weeks.8,47 A practical clinical clue is poor response to standard analgesics, reported in 86% of dissection-related headaches compared with 48% of other unusual headaches in the same cohort,8 which may help raise suspicion for an underlying vascular cause. These clinical features underscore the importance of early vascular imaging, particularly in patients presenting with isolated or atypical headache without overt neurological deficits.
1. Computed tomography angiography and magnetic resonance angiography
Although catheter angiography has historically been regarded as the reference standard, CTA and MRI/MRA now serve as the primary noninvasive imaging modalities in patients with suspected dissection.10,48 CTA is particularly effective for depicting luminal changes such as long tapering stenosis, flame-shaped occlusion, intimal flap, dissecting pseudoaneurysm, and eccentric mural thickening.10,48 In a comparative American Journal of Neuroradiology (AJNR) study by Vertinsky et al.,48 computed tomography (CT)/CTA with aortography identified more intimal flaps, pseudoaneurysms, and high-grade stenoses than MRI/MRA. On a vessel-by-vessel analysis of 25 dissected arteries, CT/CTA was the preferred diagnostic modality in 52% of vessels, with a significant preference in VADs, whereas MRI/MRA was superior for detecting acute ischemic stroke on DWI.48 These findings support meticulous CTA as the fastest and often most decisive luminal study in the acute setting, especially when vertebral dissection is suspected.
MRI/MRA remains indispensable because it combines luminal evaluation with direct VW assessment and simultaneous detection of ischemic complications.10,48 Axial T1-weighted fat-suppressed imaging is the classic sequence for demonstrating intramural hematoma as a crescentic hyperintense mural signal once methemoglobin develops, reflecting the temporal evolution of blood products within the VW.10 An important limitation is that in the first 1 to 2 days after dissection, the hematoma contains deoxyhemoglobin and appears isointense or hypointense on T1-weighted images, potentially causing a false-negative result on early MRI.8 Accordingly, a negative early T1-weighted study does not exclude dissection when clinical suspicion remains high. TOF-MRA can show long tapering stenosis, pseudoaneurysm, or the pearl-and-string appearance, but a key advantage of MRI over CTA is that it links these vascular findings to the brain parenchyma on the same examination.10,48 In the Vertinsky series, 78% of patients had acute infarction on DWI, including lesions occult or subtle on noncontrast CT.48 In practice, CTA and MRI/MRA are complementary rather than competing modalities: CTA is generally superior for defining luminal morphology, particularly in VAD, whereas MRI/MRA provides better characterization of intramural hematoma and concomitant ischemic brain injury.10,48
2. Magnetic resonance imaging and vessel wall magnetic resonance imaging
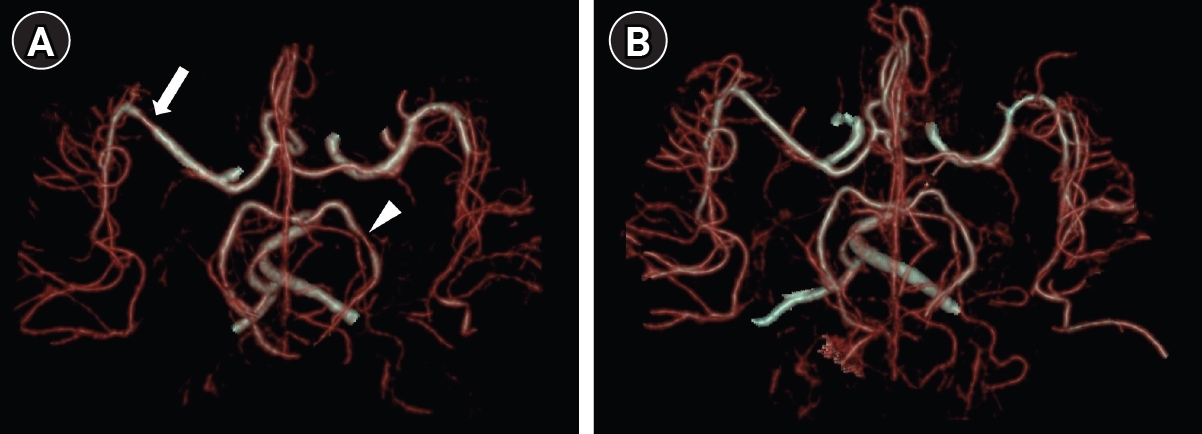
High-resolution VW-MRI complements conventional luminal imaging by directly depicting mural pathology rather than inferring it from luminal change alone.33,49 The ASNR consensus statement recommends black-blood, high-resolution, multiplanar T1-weighted pre- and post-contrast imaging, ideally at 3T, to evaluate intracranial and cervicocranial vasculopathies including dissection.33 For dissection, the most useful wall features are eccentric intramural hematoma, double lumen, intimal flap, pseudoaneurysm, and irregular luminal surface (Figure 9). This is particularly important in intracranial dissection, in which the arterial caliber is small and the classic angiographic signs may be subtle or delayed.33,46
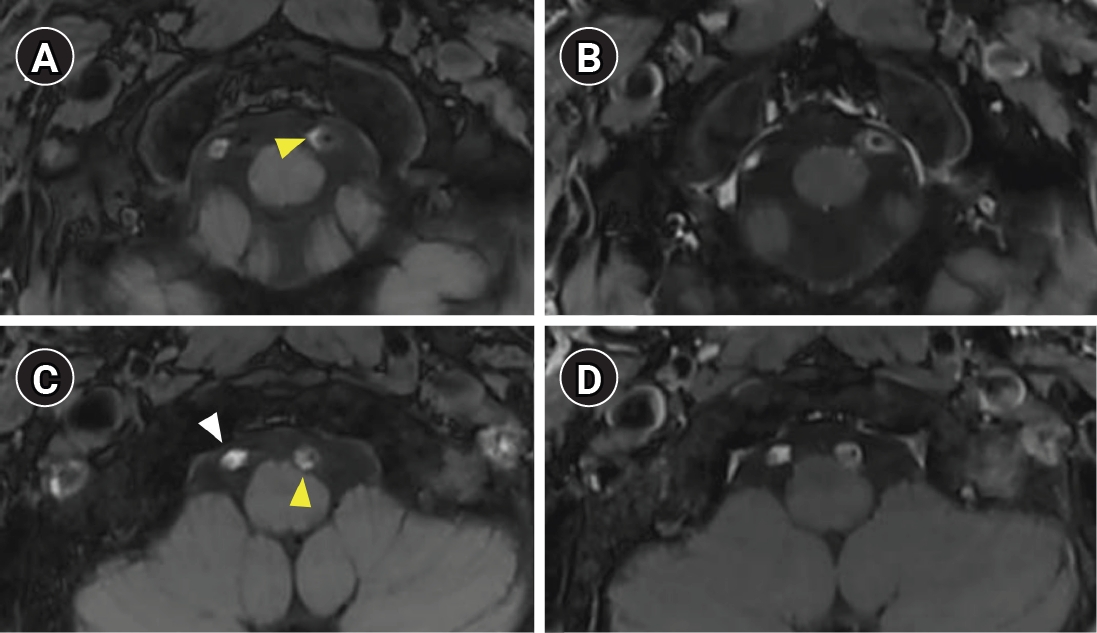
Vessel wall magnetic resonance imaging of bilateral vertebral artery dissection. (A, C) Pre-contrast T1-weighted images demonstrate intramural hematoma as a hyperintense mural signal in the left vertebral artery (yellow arrowheads). The right vertebral artery is occluded by thrombus (white arrowhead). (B, D) Contrast-enhanced T1-weighted images show no significant mural enhancement.
The most clinically relevant recent VW-MRI data come from the study by Wu et al.,49 who analyzed 145 dissected vessels in 118 patients with cervicocranial artery dissection. Compared with patients without ischemic stroke, those with stroke more often showed intramural hematoma (96.2% vs. 84.8%), irregular surface (74.7% vs. 37.9%), intraluminal thrombus (44.3% vs. 4.5%), and severe stenosis greater than 70% (54.4% vs. 31.8%).49 On multivariable analysis, irregular surface and intraluminal thrombus were independently associated with acute ischemic stroke, with odds ratios of 4.29 and 7.48, respectively.49 These findings suggest that VW-MRI is not only confirmatory but also mechanistically informative, because it helps separate relatively stable mural hematoma from unstable thromboembolic lesions that confer a higher stroke risk.
VW-MRI is also useful when dissection mimics atherosclerosis, vasculitis, or reversible vasoconstriction. In general, dissection produces a focal or segmental eccentric wall abnormality with mural hematoma or flap, rather than the plaque-like T2 hyperintensity of intracranial atherosclerosis or the diffuse inflammatory enhancement pattern of vasculitis.10,33,48,49 For headache-dominant cases with equivocal CTA or MRA, this direct wall information can be the decisive feature that keeps dissection from being misclassified as a nonspecific stenotic arteriopathy.
3. Ischemic complications
Diffusion-weighted MRI is the key parenchymal sequence for symptomatic dissection because stroke is the main determinant of early morbidity. In the imaging study by Morel et al.,50 100 of 172 consecutive patients with spontaneous cervical artery dissection (58%) had acute ischemic stroke on DWI. Importantly, the dominant mechanism was thromboembolism: 85 of 100 strokes were classified as thromboembolic, 12 as hemodynamic, and 3 as mixed.50 This explains why many infarcts in dissection appear as territorial cortical or corticosubcortical embolic lesions rather than pure watershed ischemia, although severe stenosis or occlusion can still produce hemodynamic border-zone infarction.50 This embolic-predominant pattern contrasts with the bilateral watershed distribution more characteristic of RCVS, reflecting the fundamentally different ischemic mechanisms between the two conditions. Internal carotid dissections mainly threaten the anterior circulation, whereas vertebral dissections predominantly involve the posterior circulation.43,50
These pathophysiological features have two important imaging implications. First, DWI should be obtained even when the presenting complaint is isolated unilateral headache or neck pain, because clinically silent or minimally symptomatic infarction is not rare.48,50 Second, VW features that imply luminal instability, especially irregular surface and intraluminal thrombus, should raise concern for artery-to-artery embolism and warrant closer short-term imaging and clinical surveillance.49 Intracranial artery dissection deserves separate mention because ischemic presentation can coexist with a risk of subarachnoid hemorrhage, particularly in dissecting aneurysmal lesions of the posterior circulation.46,51 In such cases, imaging may reveal basal cistern or perimesencephalic subarachnoid hemorrhage in association with fusiform or irregular aneurysmal dilatation of the affected intracranial artery, findings that should prompt consideration of endovascular or surgical intervention to prevent rebleeding.46
4. Follow-up imaging
Serial imaging is an integral part of dissection management because both the mural hematoma and the lumen evolve substantially over time.43,45,51,52 Healing and arterial remodeling often occur during the first 3 to 6 months, whereas persistent pseudoaneurysm or residual stenosis may remain and influence subsequent management.45,51,52 In a population-based cohort by Griffin et al.,44 follow-up imaging showed near-complete or complete luminal resolution in 53.2% of patients, stable residual abnormality in 45.9%, and new pseudoaneurysm formation in 6.4%, underscoring the importance of serial vascular imaging. Contemporary guidelines from the European Stroke Organisation and the American Heart Association both support repeat noninvasive vascular imaging after the acute phase to document vessel healing, persistent abnormality, or interval aneurysmal change.51,52 In practical terms, MRI/MRA is preferred when mural hematoma resolution is important, whereas CTA remains useful when the key question is residual stenosis, pseudoaneurysm, or vertebral artery lumen morphology (Figure 10). The temporal pattern of dissection imaging—early false-negative T1, mural hematoma evolution, and luminal remodeling—is summarized alongside RCVS and CVT in Table 2.
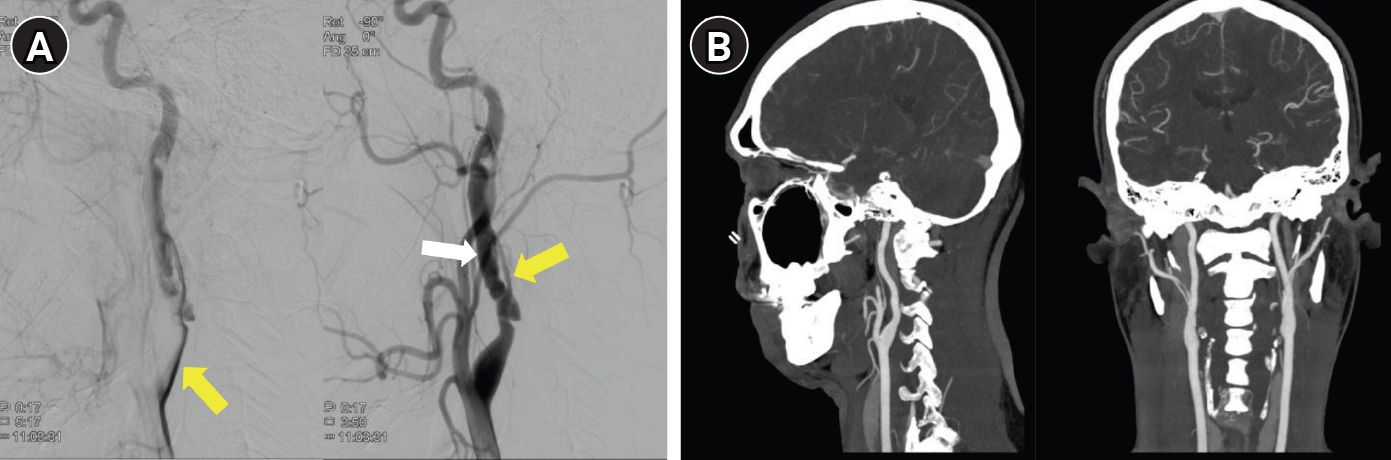
Right cervical internal carotid artery (ICA) dissection with long-term follow-up. (A) Initial digital subtraction angiography demonstrates a markedly narrowed true lumen (yellow arrows) and false lumen (white arrow) of the right cervical ICA, consistent with acute dissection. (B) Follow-up computed tomography angiography at 6 years shows complete resolution of the dissection with normalization of the arterial lumen.
The follow-up goal differs slightly by subtype. In extracranial dissection, the main task is to confirm remodeling or stable residual abnormality. In intracranial dissection, follow-up is often more diagnostic, because interval fusiform dilatation, mural hematoma evolution, or aneurysmal transformation can clarify a lesion that was initially indeterminate.46,51 For headache specialists and stroke imagers alike, the main lesson is that a single study can establish suspicion, but interval imaging often establishes certainty.
CEREBRAL VENOUS THROMBOSIS
CVT refers to thrombosis of the dural venous sinuses, the cerebral veins, or both.53 Although it accounts for only 0.5% to 3% of all strokes, it disproportionately affects young adults, women of reproductive age, and patients with prothrombotic conditions.53 From the perspective of a headache imaging review, CVT is especially important because headache is usually the first symptom and may occur in the absence of focal deficits or overt intracranial hypertension.5,53 This clinical variability makes neuroimaging decisive: the diagnosis is rarely secured by symptoms alone and instead relies on imaging patterns that integrate direct thrombus visualization with venous flow disturbance and parenchymal injury.
Modern imaging-based reviews show that headache occurs in approximately 89% to 91% of patients with CVT, whereas focal deficits and seizures occur in 52% to 68% and 39% to 44%, respectively.54 The prospective series by Cumurciuc et al.9 highlights the headache-predominant end of the spectrum: among 123 consecutive patients with CVT, 17 presented with isolated headache and normal CT and CSF findings; 3 of the 17 had TCH. Prognosis is often favorable with prompt diagnosis and anticoagulation, but not uniformly so. In the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT), 57.1% of patients were symptom-free at follow-up, whereas 8.3% died; deep venous thrombosis and hemorrhage on admission imaging predicted worse outcome.55 The imaging task is therefore twofold: to detect thrombosis early and to distinguish potentially reversible venous edema from irreversible venous infarction.
1. Noncontrast computed tomography and computed tomography venography
Noncontrast CT is usually the first examination obtained in acute headache or stroke pathways and therefore remains central to the initial detection of CVT.11,53,54 It may be normal, but when abnormal it can show direct thrombus signs such as a hyperdense cortical vein or dural sinus, the dense triangle sign in the superior sagittal sinus, or indirect parenchymal consequences such as venous edema, hemorrhagic venous infarction, or convexity subarachnoid hemorrhage.11,54 The important pitfall is that normal CT does not exclude CVT, particularly in isolated headache or isolated cortical vein thrombosis (ICoVT). This reflects both the temporal evolution of thrombus density and the limited sensitivity of CT for ICoVT.
CTV is the fastest confirmatory venous study in many emergency settings. According to the 2024 American Heart Association statement, CT and MRI are the main imaging modalities, and CTV or magnetic resonance venography (MRV) are the optimal tests to confirm CVT.53 Typical CTV findings include a persistent intraluminal filling defect, non-opacification of the thrombosed sinus, and the empty delta sign in superior sagittal sinus thrombosis.11,54 CTV is particularly useful when CVT enters the differential diagnosis after a noncontrast CT obtained for TCH, lobar hemorrhage, or unexplained edema. Its main limitations are lower sensitivity for ICoVT and the need to distinguish true filling defects from normal venous variants, especially asymmetric transverse sinus hypoplasia.11,54
2. Magnetic resonance imaging and magnetic resonance venography
MRI is the most sensitive imaging technique for CVT because it combines direct thrombus assessment, venous flow evaluation, and parenchymal characterization in a single study.11,54 Standard T1-, T2-, FLAIR-, and diffusion-weighted sequences remain useful, but their direct clot signal depends on thrombus age and can therefore be misleading if interpreted in isolation.11 CE-MRV is generally the most accurate magnetic resonance (MR) venographic technique, whereas TOF-MRV is more vulnerable to slow flow, in-plane saturation, and congenital hypoplasia.11,54 For this reason, direct sinus or vein signal on MRI and venographic flow information should be interpreted together rather than as separate tests.
Susceptibility-sensitive imaging has become particularly important. In the Stroke study by Idbaih et al.,56 114 MRI examinations from 39 patients with CVT were analyzed, including 166 clots. The sensitivity of T2* SWI for thrombus detection was 90% during days 1 to 3, outperforming conventional sequences in the acute phase, and remained relatively stable during the first week.56 For cortical venous thrombosis, T2* SWI detected 97% of thrombosed cortical veins, compared with 78% for T1 spin-echo and less than 40% for FLAIR or DWI.56 These data support the routine inclusion of susceptibility-sensitive sequences (SWI or GRE) in MRI protocols for suspected CVT, particularly when cortical vein thrombosis or very early thrombosis is a concern (Figure 11).
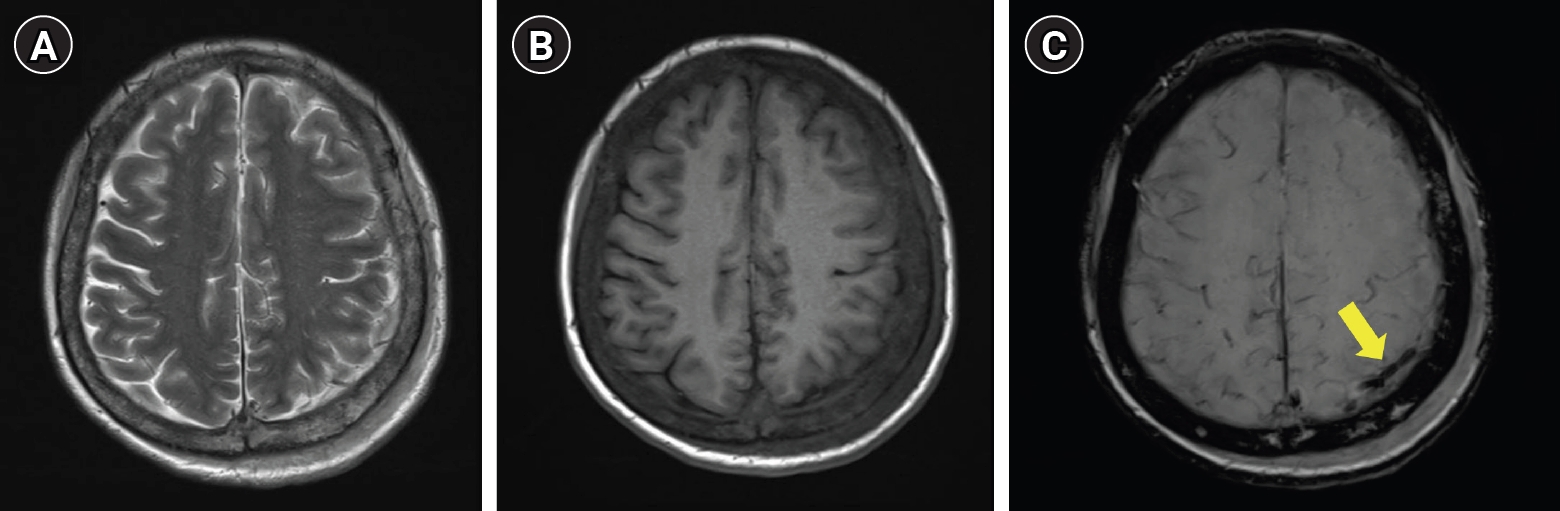
Isolated cortical vein thrombosis on multimodal magnetic resonance imaging (MRI). Brain MRI was obtained 2 days after the onset of aphasia and right hemiparesis. (A) Axial T2-weighted image at the level of the affected cortex shows no definite abnormality. (B) Corresponding axial T1-weighted image is similarly unremarkable. (C) Axial susceptibility-weighted image at the same level demonstrates a linear hypointense signal along a left cortical vein (yellow arrow), consistent with thrombosis and reflecting the susceptibility effect of deoxygenated blood within the occluded vessel. This figure illustrates that cortical vein thrombosis may be occult on conventional T1- and T2-weighted images but detectable on susceptibility-sensitive imaging.
This is even more relevant in ICoVT, a distinct but easily missed subtype of venous thrombosis. In the systematic review by Coutinho et al.,57 116 published cases were identified; mean age was 41 years and 68% of patients were women. In the dedicated MR follow-up study by Boukobza et al.,58 all 8 patients with ICoVT showed a magnetic susceptibility effect in the thrombosed cortical vein on T2* GRE imaging at diagnosis. MRV was performed in all patients, but after the clot was recognized on T2* imaging, definite venous occlusion on MRV became apparent in only a subset, underscoring that MRV alone may miss ICoVT.58 Adjacent parenchymal FLAIR and DWI abnormalities were present in 6 of 8 patients, and petechial hemorrhage or hematoma was present in 5 of 8.58 For headache-dominant patients with a negative or equivocal MRV, susceptibility-sensitive imaging is therefore often the decisive sequence.
Methemoglobin-sensitive clot imaging techniques, conceptually related to MR direct thrombus imaging, further emphasize direct visualization of thrombus rather than inference from absent flow.11,56 However, in current clinical practice, the most mature and widely available approach remains the combination of standard MRI, susceptibility-sensitive sequences, and venography.11,54,56
3. Parenchymal complications
Venous parenchymal injury differs fundamentally from arterial infarction because the lesion distribution follows venous drainage rather than arterial territories.11,54,59 In the diffusion-weighted MRI study by Mullins et al.,59 superficial CVT was associated with cortical and subcortical abnormalities, whereas deep venous thrombosis was associated with deep gray nucleus and deep white matter lesions. This topographic rule is highly practical: bilateral thalamic edema or hemorrhage should immediately raise suspicion for deep venous thrombosis, while parasagittal or lobar corticosubcortical lesions suggest superficial sinus or cortical vein involvement.
Mullins et al.59 also clarified that venous parenchymal lesions are biologically heterogeneous on DWI and apparent diffusion coefficient. Three lesion patterns were identified: lesions with elevated diffusion that later resolved, consistent with vasogenic edema; lesions with low diffusion that persisted, consistent with cytotoxic injury; and lesions with low diffusion that resolved in patients with seizure activity.59 This is important because restricted diffusion in CVT does not necessarily imply irreversible arterial-type infarction. Venous lesions can be mixed, partially reversible, and accompanied by hemorrhage. Accordingly, hemorrhagic venous infarction, lobar intracerebral hemorrhage, and localized convexity subarachnoid hemorrhage should all prompt evaluation of the venous system rather than automatic attribution to primary hemorrhagic stroke.11,54,59
At the prognostic level, the ISCVT study showed that hemorrhage on admission CT and thrombosis of the deep cerebral venous system independently predicted death or dependence.55 Thus, parenchymal imaging in CVT is not just descriptive; it identifies the subgroup in whom a typically favorable disease becomes potentially malignant.
4. Follow-up imaging
Follow-up imaging in CVT serves two purposes: documenting recanalization and clarifying the evolution of parenchymal lesions or residual cortical vein abnormality.11,53,58,60 In the prospective study by Stolz et al.,60 37 patients with dural sinus thrombosis underwent serial vascular imaging. Recanalization was already present in 60% at hospital discharge after a mean of 22±6 days, and rates increased thereafter, although early recanalization was not clearly linked to functional outcome.60 These data support the common practice of repeat venous imaging during the first weeks to months after diagnosis, while also reminding clinicians that radiographic reopening and clinical recovery are related but not interchangeable endpoints (Figure 12). Table 2 places this recanalization pattern in context alongside the temporal evolution of imaging findings in RCVS and arterial dissection.
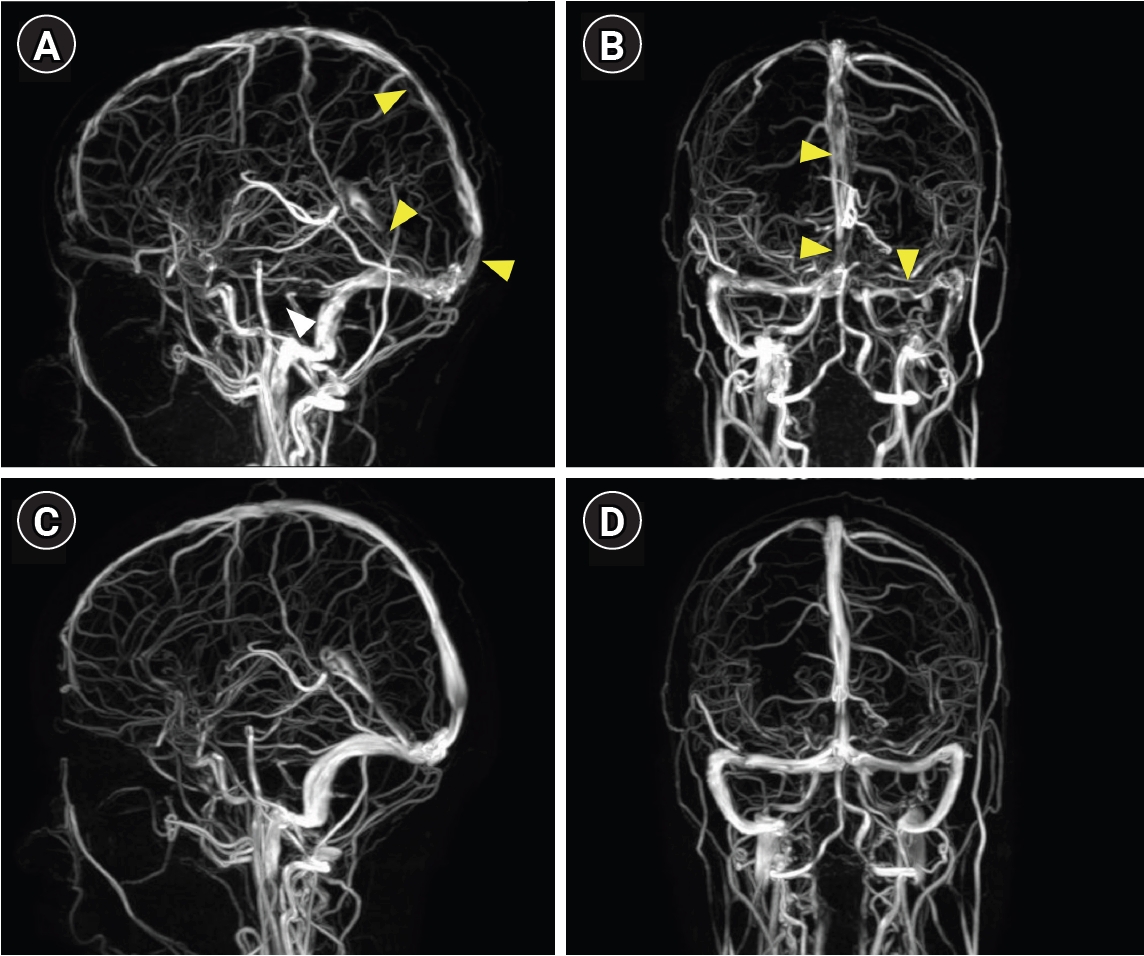
Cerebral venous thrombosis with follow-up magnetic resonance venography (MRV) after anticoagulation. (A, B) Initial MRV demonstrates filling defects in the superior sagittal sinus, with nonvisualization of the transverse sinus and straight sinus (yellow arrowheads), consistent with multisinus thrombosis. (C, D) Follow-up MRV at 1 month after initiation of anticoagulation therapy shows substantial recanalization of the affected sinuses.
Follow-up MRI is especially valuable in ICoVT, where susceptibility-sensitive abnormalities may persist longer than abnormalities on conventional sequences. In the Boukobza series, T2* abnormalities remained detectable on follow-up examinations up to 18 months, whereas signal abnormalities on T1-, T2-, FLAIR-, and DWI sequences regressed much earlier.58 In other words, a residual susceptibility abnormality does not necessarily indicate active thrombosis, and serial interpretation must be anchored to the full imaging context. For routine practice, CTV or MRV is generally used to document sinus recanalization, whereas susceptibility-sensitive MRI is particularly helpful when cortical vein thrombosis or prior hemorrhagic residue remains in question.11,53,58,60
INTEGRATED DIAGNOSTIC PEARLS AND PITFALLS
The key practical imaging pearls and pitfalls of RCVS, arterial dissection, and CVT—together with the diagnostic context in which each pitfall arises and the role of follow-up imaging—are summarized in Table 3.
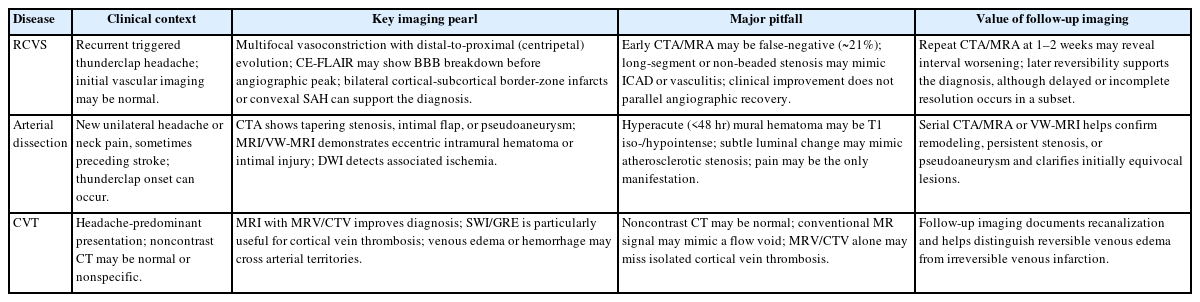
Key diagnostic imaging pearls and pitfalls in RCVS, arterial dissection, and CVT
CONCLUSION
RCVS, cervical and intracranial artery dissection, and CVT are three cerebrovascular disorders that share a common clinical feature: headache is frequently the earliest or sole presenting symptom, often preceding neurological deficits and occurring at a stage when neuroimaging may be normal or nonspecific. This review highlights that each condition poses distinct but overlapping diagnostic challenges that can be addressed through a structured, multimodal imaging approach.
Across these three entities, no single imaging modality is sufficient for definitive diagnosis. Luminal imaging techniques such as CTA and MRA define vascular caliber and detect stenosis, occlusion, or vasoconstriction, whereas MRI provides critical information on parenchymal injury and direct visualization of mural or thrombus pathology. Advanced techniques—including high-resolution VW-MRI, CE-FLAIR, and SWI—have expanded the diagnostic toolkit by revealing VW changes, BBB disruption, and early thrombus that may be occult on conventional studies.
Equally important is the temporal dimension of imaging. In RCVS, vasoconstriction may be confined to distal vessels below angiographic resolution during the first week; in dissection, intramural hematoma can be isointense on early T1-weighted imaging; and in CVT, acute thrombus may mimic a normal flow void on conventional MRI. These pitfalls underscore the need for repeat imaging when clinical suspicion persists despite initially unremarkable studies. Moreover, the temporal evolution of imaging findings is itself diagnostically informative: the centripetal propagation of vasoconstriction in RCVS, the remodeling of mural hematoma in dissection, and the progression of venous recanalization in CVT each provide interval data that can confirm or refine an initially uncertain diagnosis.
In this context, the role of neuroimaging extends beyond diagnosis alone: it serves as a tool for risk stratification, differentiation of overlapping arteriopathies, and monitoring of disease evolution. For clinicians evaluating patients with new, severe, or atypical headache, an imaging strategy that integrates appropriate modality selection, sequence optimization, and timely follow-up remains essential for early and accurate diagnosis of these important cerebrovascular causes of secondary headache.
Notes
AVAILABILITY OF DATA AND MATERIAL
The data presented in this study are available upon reasonable request from the corresponding author.
AUTHOR CONTRIBUTIONS
Conceptualization: YEG; Writing–original draft: YEG; Writing–review & editing: YEG.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING STATEMENT
None.
ACKNOWLEDGMENTS
None.