Menstrual Migraine: A Review of Current Research and Clinical Challenges
Article information

Abstract
The term “menstrual migraine” is commonly used to describe migraines that occur in association with menstruation, as distinct from other migraine types. A significant proportion of women of reproductive age experience migraine attacks related to their menstrual cycle. Menstrual migraine is characterized by migraine attacks occurring on day 1±2 (i.e., days −2 to +3) of menstruation in at least two out of three menstrual cycles. Although the reported prevalence of menstrual migraine varies considerably, population-based studies have found that menstrual migraine affects up to 60% of women with migraines. Several hypotheses have been proposed to explain the etiology of menstrual migraine, among which the estrogen withdrawal hypothesis is the most widely accepted. Women who experience menstrual migraines often face considerable disability due to perimenstrual attacks. Studies have reported that perimenstrual attacks are more severe and more difficult to manage than nonmenstrual attacks. The principles of acute managing perimenstrual attacks are the same as those for managing nonmenstrual attacks. Short-term preventive therapy is needed to prevent menstrual migraines before they occur during the perimenstrual period. This review summarizes the prevalence, distinct clinical features, pathophysiological mechanisms, and management of menstrual migraine.
INTRODUCTION
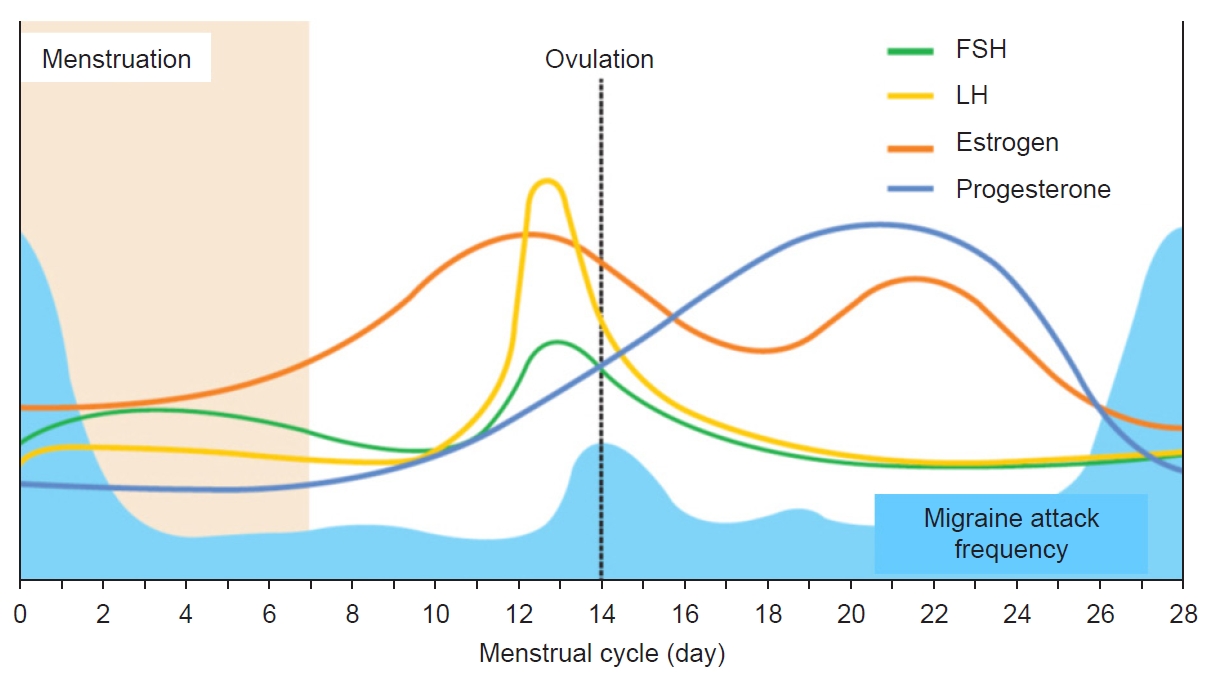
Migraine is a disabling neurological disease that affects 14% of the world’s population at all ages.1 Characteristic features include recurrent attacks of severe headache and accompanying symptoms such as nausea or vomiting, photophobia, and phonophobia.2 Prevalence substantially varies with age and sex, and it affects 2–3 times more women than men. A significant number of women of reproductive age report migraine attacks related to the menstrual cycle (Figure 1).3-6 Several mechanisms including hormonal effects have been proposed to explain menstruation-related migraine in women,5 however, the exact underlying pathophysiological mechanisms remain poorly understood.
Many women with migraine meet the criteria for menstrually related migraine or pure menstrual migraine. Menstrual migraine can be used to describe a condition in which migraine attacks occur on day 1±2 (i.e., days −2 to +3) of menstruation in at least two out of three menstrual cycles.7
In women who have menstrual migraine, perimenstrual attacks are associated with considerable disability. However, in clinical practice, menstrual migraine is less well-recognized and managed. This review elucidates the prevalence, clinical features, pathophysiological mechanisms, and management of menstrual migraine.
PREVALENCE
Due to the paucity of data, and differences in the study design, population, and case definitions, there are large variations in the prevalence of menstrual migraine. Population-based studies have reported menstrual migraine affecting up to 60% of females with migraine, however, the definition of the perimenstrual period was broader than 5 days.8,9 Another population-based studies with stricter criteria reported that 4% to 8% of all women and 18% to 25% of females with migraine have menstrual migraine without aura.10-12 In the general population, the prevalence of menstrual migraine with aura has been estimated to be 1.7% to 8.1% of females with migraine.10,11,13 In patients from headache clinics, the prevalence of menstrual migraine without aura is higher, varying from 22% to 70%.14-16 The discrepancy between clinic-based and population-based studies might be a diagnostic criterion because women visiting headache clinics have a higher frequency of migraine.
A recent clinic-based study found that the accuracy of self-reported menstrual migraine is poor, compared with a diary-based diagnosis.7 Furthermore, most clinical studies on menstrual migraine use different definitions of menstrual migraine. For example, in some studies, the perimenstrual period is extended by several days, whereas the definition of the perimenstrual period is nonexistent in others.15,16 Clinical studies with the highest prevalence have looser definitions of menstrual migraine and extended perimenstrual windows, increasing the likelihood that a migraine will be classified as menstrual by chance. In addition, the current diagnostic criteria in the International Classification of Headache Disorders, third edition (ICHD-3) for menstrual migraine have several issues that need to be informed (Table 1).7 First, the diagnostic criteria does not consider migraine frequency. Diagnostic misclassification of menstrually related migraine may occur in women with high frequency episodic migraine or chronic migraine, because women with 8 or more migraine days per month may have high probability of migraine attacks within 5-day perimenstrual window. Second, women with rare migraine attacks occurring exclusively at menstruation do not fulfill the diagnostic criteria because the rare migraine attack frequency does not reach 2 of 3 consecutive menstrual cycle. Third, timing of migraine attacks is currently unclear what is meant by ‘occur’ in the diagnostic criteria. Meaning of ‘occur’ is not clear whether it means migraine attacks begin and/or end on day 1±2 of menstruation. There issues have been discussed in other study.17

CLINICAL FEATURES
Menstrual migraine have similar clinical features compared to migraine unrelated to the menstrual cycle, but tend to be differ in the severity of symptoms or treatment response. No differences in the characteristics of perimenstrual attacks compared with attacks at other times of the cycle were reported in some studies, whereas other studies report that perimenstrual attacks are more severe and more difficult to manage than nonmenstrual attacks.3,4,18,19 Studies using headache and menstruation diary report that perimenstrual attacks are more disabling and can persist for up to 35% longer than those unrelated to the menstrual cycle.20-24 Moreover, perimenstrual attacks are associated with more severe pain and accentuated associated symptoms such as photophobia and phonophobia.20 The drug response to triptans also seems to differ between perimenstrual attacks and those unrelated to the menstrual cycle, with the former having a higher recurrence rate of attacks after acute medical treatment.20
DIAGNOSIS
For all types of migraine, menstrual migraine is a commonly used term occurring in association with menstruation. The diagnostic criteria of menstrual migraine have been included in the International Classification of Headache Disorders since its 2nd edition,25 in which appendix criteria were outlined for two types of menstrual migraine without aura: “pure menstrual migraine” and “menstrually-related migraine”. The ICHD-3 included the addition of criteria for menstrual migraine with or without aura.26 Table 1 illustrates the appendix criteria for pure menstrual migraine and menstrually-related migraine, as described in the ICHD-3 from 2018.26 A potential overestimation of perimenstrual attacks might occur by chance in all women affected by migraines, and can be mistaken for menstrual migraine. A headache and menstruation diary may help to confirm the diagnosis because studies indicate that women tend to overreport an association between migraine and menstruation.27,28
PATHOPHYSIOLOGY
Several hypotheses have been proposed to explain the etiology of menstrual migraine, with the estrogen withdrawal hypothesis as the most widely accepted.29 The premenstrual phase of the menstrual cycle is characterized by declining plasma estrogen levels.29 The estrogen withdrawal hypothesis was first introduced by Somerville29 in 1972. The study results demonstrated that the expected onset of migraine had seemingly been delayed by a few days following the injection of estradiol. His studies suggest that a precipitous drop in estrogen shortly before menstruation increases the risk of developing a migraine attack.29-31 In a series of small studies, a premenstrual drop in estrogen was consistently associated with migraine.32 This hypothesis was supported by a larger study, which revealed that the incidence of migraine without aura, but not migraine with aura, was inversely associated with urinary estrogen concentrations across the menstrual cycle.5 In general, female sex hormones can modulate the activity of several neurotransmitter systems involved in the migraine pathophysiology and pain transmission.33 Estrogen modulates the activity in the µ-opioid system. Late luteal low estrogen is associated with a reduced capacity to activate the µ-opioid system, resulting in a state of susceptibility to pain.33 Estrogen can also modulate the serotonergic system activity, and a change in the serotonergic tone accompanying estrogen withdrawal has been proposed as a possible trigger of attacks.34
In addition to its effects on neurotransmission, estrogen can regulate the sensitization of trigeminal neurons by modulating the release of neuropeptides such as calcitonin gene-related peptide (CGRP).35 In some in vitro animal studies, estradiol was found to reduce CGRP expression in the trigeminal ganglion.35 The relationship between estrogen and CGRP levels in humans remains unclear, as studies have produced conflicting evidence. A study reported higher interictal plasma CGRP concentrations in women with menstrually related migraine during menstruation than in healthy women, which could explain their heightened susceptibility to migraine during the perimenstrual period.36
Some studies suggest that genetic factors may be involved in menstrual migraine.37 Genetics may indeed regulate individual-level sensitivity to estrogen fluctuations, rendering some women more susceptible to menstrual migraine.37 The current evidence is conflicting. Limited evidence exists for the role of genetics in menstrual migraine. Candidate gene association studies evaluated the role of estrogen receptor 1 gene (ESR-1),38 which mediates estradiol activity. The COMT, CYP1A1, and CYP19A1 genes, which are involved in estradiol synthesis and metabolism, has been a further focus of research.39 Although a British and Italian study reported no significant difference in functional polymorphisms of estrogen synthesis and metabolism genes,39,40 an American study identified one COMT polymorphism and two tyrosine hydroxylase gene polymorphisms linked to self-reported menstrual migraine.41 Furthermore, two ESR-1 polymorphisms were associated with menstrual migraine in the Chinese and Turkish cohorts.42,43 Because each identified genetic variant is likely to account for modest effects in increasing the risk of menstrual migraine, further research is warranted to understand the role of genetics in menstrual migraine.
MANAGEMENT
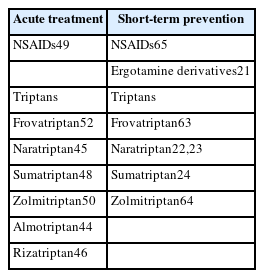
Acute and preventive (short-term or standard) treatments were summarized in Table 2.
Pharmacological treatments for menstrual migraine
1. Acute treatment
The principles of managing perimenstrual attacks are the same as those for managing nonmenstrual attacks. Drugs used for the acute treatment of nonmenstrual migraine attacks are also effective for perimenstrual migraine.28,44-51 Studies for the acute management of menstrual migraine have shown that most triptans are effective in reducing pain associated with menstrual migraine. Positive clinical evidence exists for almotriptan,44 frovatriptan,52 naratriptan,45 rizatriptan,46 sumatriptan,48 and zolmitriptan.50 However, some clinical trials have shown that perimenstrual attacks in women diagnosed with menstrual migraine do not respond as well to acute treatment as do their attacks outside of this period.24,28 Perimenstrual attacks last longer than attacks at other times of the menstrual cycle,22,23,53 therefore, treatment is usually necessary for several days. Some studies compared frovatriptan which has a long elimination half-life of 26 hours with almotriptan, rizatriptan, or zolmitriptan for the treatment of perimenstrual attacks in women diagnosed with menstrual migraine.22,23,54 The results demonstrated similar efficacy for a 2 hours pain relief, pain-free response, and sustained pain absence at 48 hours, however, the recurrence rate (pain free at 2 hours with headache of any severity returning within 24 hours) was significantly lower with frovatriptan than with the comparators. This result suggests that frovatriptan may more appropriate than other triptans for the acute treatment of perimenstrual migraine attacks. Nonsteroidal antiinflammatory drugs, alone or together with triptans,49,55-57 and combination analgesics have also been proven effective for the acute treatment of menstrual migraine.58 Recent study showed that lasmiditan was effective for treatment of menstrual migraine.59
2. Prophylactic treatment
1) Standard prophylaxis
There are no strong evidence suggesting potential efficacy in menstrual migraine. Randomized, prospective, placebo-controlled trials, assessing the efficacy of standard long-term migraine preventive therapies for menstrual migraine are clearly needed. However, in the absence of these trials, it may be helpful to try medications already established as effective for migraine prevention. Effective migraine preventive therapies include topiramate, divalproex sodium, propranolol, and timolol.58 Hormonal preventive therapy using contraceptive was effective to reducing migraine frequency in women with menstrual migraine.60 Recent study revealed that prophylactic use of anti-CGRP antibodies for women with menstrual migraine leads to reductions in migraine days during menstrual cycle.61
2) Short-term prevention of menstrual migraine.
The goal of the short-term preventive therapy is to prevent menstrual migraine headaches before they occur. Treatment is usually initiated several days before the expected onset of the perimenstrual attack to achieve a steady state of medication, although this schedule relies on the woman being able to predict the onset of menstruation, perimenstrual attacks, or both.
Clinical trial data for perimenstrual prophylaxis with nonsteroidal antiinflammatory drugs and triptans are available. Several studies have shown short-term prevention to be an effective treatment with naratriptan,22,23 frovatriptan,62 and oral sumatriptan.24 Frovatripan 2.5 mg once daily and twice daily were effective in perimenstrual prophylaxis.63 In this study, patients were treated during perimenstrual periods (start taking it 2 days before menstruation is expected and continue for 6 days).63 Treatment began with a double-loading dose of study medication on day 1.63 A systematic review and meta-analysis of triptans used for the prevention of perimenstrual attacks of migraine concluded that frovatriptan 2.5 mg twice daily and zolmitriptan 2.5 mg three times daily were the most effective and best tolerated perimenstrual regimens.64 Naproxen sodium has been demonstrated to be effective for short-term prevention of migraine65 and a number of other nonsteroidal antiinflammatory agents have been suggested to be effective when studied in smaller clinical trials.20,58 Dihydroergotamine mesylate administered as a nasal spray for 6 days starting 2 days before the expected onset of headache in 40 women with menstrual migraine was demonstrated to reduce menstrual migraine severity.21
CONCLUSIONS
In women diagnosed with migraine, menstrual migraine is common and is associated with considerable disability. Although pathophysiological mechanisms remain to be explored, several mechanisms such as the estrogen withdrawal hypothesis, CGRP release, and genetic factors have been proposed to explain menstrual migraine. In women diagnosed with menstrual migraine, perimenstrual attacks differ in duration, severity, and response to treatment compared with nonmenstrual migraine attacks. If menstrual migraine persists despite standard prophylaxis, or if the response to acute treatment is inadequate, short-term perimenstrual prophylaxis should be considered. Menstrual migraine is overreported when the diagnoses are based on self-reports. Therefore, further studies are warranted to use a prospective headache and menstruation diary to confirm the diagnosis in clinical trials.
Notes
Availability of data and material
Not applicable.
Author contributions
Conceptualization, Data curation, Formal analysis, Writing–original draft, Writing–review and editing: JGS.
Conflict of interest
Jong-Geun Seo is the Editor of Headache and Pain Research and was not involved in the review process of this article. Author has no other conflicts of interest to declare.
Funding statement
Not applicable.
Acknowledgments
Not applicable.