
Articles
- Page Path
- HOME > Headache Pain Res > Volume 27(1); 2026 > Article
-
Review Article
Alcohol-Induced Headache: A Narrative Review Based on Migraine Pathophysiology -
Woo-Seok Ha

-
Headache and Pain Research 2026;27(1):21-29.
DOI: https://doi.org/10.62087/hpr.2025.0027
Published online: February 23, 2026
Department of Neurology, Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea
- Correspondence: Woo-Seok Ha, M.D. Department of Neurology, Severance Hospital, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Republic of Korea Tel: +82-2-2228-1600, Fax: +82-2-393-0705, E-mail: haha88@yuhs.ac
© 2026 The Korean Headache Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 5,579 Views
- 31 Download
Abstract
- Alcohol-induced headache (AIH) is one of the most common headache experiences and is associated with a substantial socioeconomic burden; however, its pathophysiological mechanisms and clinical classification remain inadequately defined. Accumulating evidence indicates that AIH shares key biological pathways with migraine, particularly involving activation of the trigeminovascular system and calcitonin gene-related peptide (CGRP) signaling. Although currently available hangover remedies are supported by limited high-quality evidence, anti-CGRP treatments have emerged as a biologically plausible option for the situational prevention and acute treatment of AIH. A phenotype-based approach is therefore essential for achieving accurate diagnosis and effective management of alcohol-related headaches. Future well-designed clinical trials focusing on CGRP antagonists are warranted to address this common yet neglected disorder.
INTRODUCTION
CLINICAL PHENOTYPES AND CLASSIFICATIONS
EPIDEMIOLOGICAL ASSOCIATIONS WITH PRIMARY HEADACHES AND SUSCEPTIBILITY
PATHOPHYSIOLOGICAL MECHANISMS LINKING ALCOHOL AND MIGRAINE
CURRENT EVIDENCE AND THERAPEUTIC CONSIDERATIONS
CONCLUSIONS
AVAILABILITY OF DATA AND MATERIAL
Not applicable.
AUTHOR CONTRIBUTIONS
Conceptualization: WSH; Writing–original draft: WSH; Writing–review & editing: WSH.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING STATEMENT
Not applicable.
ACKNOWLEDGMENTS
Not applicable.
- 1. Rasmussen BK, Olesen J. Symptomatic and nonsymptomatic headaches in a general population. Neurology 1992;42:1225-1231.ArticlePubMed
- 2. Severeijns NR, Sips ASM, Merlo A, Bruce G, Verster JC. Absenteeism, presenteeism, and the economic costs of alcohol hangover in the Netherlands. Healthcare (Basel) 2024;12:335.ArticlePubMedPMC
- 3. Verster JC, Penning R. Treatment and prevention of alcohol hangover. Curr Drug Abuse Rev 2010;3:103-109.ArticlePubMed
- 4. Liu L, Wang J, Rosenberg D, Zhao H, Lengyel G, Nadel D. Fermented beverage and food storage in 13,000 y-old stone mortars at Raqefet Cave, Israel: investigating Natufian ritual feasting. J Archaeol Sci Rep 2018;21:783-793.Article
- 5. Zarshenas MM, Petramfar P, Firoozabadi A, Moein MR, Mohagheghzadeh A. Types of headache and those remedies in traditional persian medicine. Pharmacogn Rev 2013;7:17-26.ArticlePubMedPMC
- 6. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia 2004;24 Suppl 1:9-160.ArticlePubMed
- 7. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018;38:1-211.ArticlePubMedPMCPDF
- 8. Dueland AN. Headache and alcohol. Headache 2015;55:1045-1049.ArticlePubMed
- 9. Evans RW, Sun C, Lay C. Alcohol hangover headache. Headache 2007;47:277-279.ArticlePubMed
- 10. Hindiyeh NA, Zhang N, Farrar M, Banerjee P, Lombard L, Aurora SK. The role of diet and nutrition in migraine triggers and treatment: a systematic literature review. Headache 2020;60:1300-1316.ArticlePubMedPMCPDF
- 11. Kim BK, Bae HJ, Koo JS, Kwon OH, Park JM. Clinical characteristics of migraine and tension-type headache: the experience in Eulji Hospital. Korean J Headache 2005;6:103.
- 12. Syapin PJ. Alcohol and nitric oxide production by cells of the brain. Alcohol 1998;16:159-165.ArticlePubMed
- 13. Hakim SM. The potential role of calcitonin gene-related peptide antagonists for the management of hangover headaches. Curr Opin Anaesthesiol 2025;38:669-673.Article
- 14. Nicoletti P, Trevisani M, Manconi M, et al. Ethanol causes neurogenic vasodilation by TRPV1 activation and CGRP release in the trigeminovascular system of the guinea pig. Cephalalgia 2008;28:9-17.ArticlePDF
- 15. García-Azorín D, Aparicio-Cordero L, Talavera B, Johnson A, Schytz HW, Guerrero-Peral ÁL. Clinical characterization of delayed alcohol-induced headache: a study of 1,108 participants. Neurology 2020;95:e2161-e2169.ArticlePubMed
- 16. Penning R, van Nuland M, Fliervoet LA, Olivier B, Verster JC. The pathology of alcohol hangover. Curr Drug Abuse Rev 2010;3:68-75.ArticlePubMed
- 17. Ylikahri RH, Leino T, Huttunen MO, Pösö AR, Eriksson CJP, Nikkilä EA. Effects of fructose and glucose on ethanol-induced metabolic changes and on the intensity of alcohol intoxication and hangover. Eur J Clin Invest 1976;6:93-102.ArticlePubMed
- 18. Penning R, de Haan L, Verster JC. Caffeinated drinks, alcohol consumption, and hangover severity. Open Neuropsychopharmacol J 2011;4:36-39.Article
- 19. Gullberg RG. Estimating the uncertainty associated with Widmark’s equation as commonly applied in forensic toxicology. Forensic Sci Int 2007;172:33-39.ArticlePubMed
- 20. Park JW, Chu MK, Kim JM, Park SG, Cho SJ. Analysis of trigger factors in episodic migraineurs using a smartphone headache diary applications. PLoS One 2016;11:e0149577.ArticlePubMedPMC
- 21. Aamodt AH, Stovner LJ, Hagen K, Bråthen G, Zwart J. Headache prevalence related to smoking and alcohol use. The Head-HUNT Study. Eur J Neurol 2006;13:1233-1238.ArticlePubMed
- 22. Le H, Tfelt-Hansen P, Skytthe A, Kyvik KO, Olesen J. Association between migraine, lifestyle and socioeconomic factors: a population-based cross-sectional study. J Headache Pain 2011;12:157-172.ArticlePubMedPMCPDF
- 23. Tang Y, Zhang K, Zhang Y, et al. Association between dietary alcohol intake and migraine or severe headache miscellaneous pain: the NHANES 1999-2004. Brain Behav 2025;15:e70400.ArticlePubMedPMC
- 24. Błaszczyk B, Straburzyński M, Więckiewicz M, et al. Relationship between alcohol and primary headaches: a systematic review and meta-analysis. J Headache Pain 2023;24:116.ArticlePubMedPMC
- 25. Panconesi A. Alcohol and migraine: trigger factor, consumption, mechanisms. A review. J Headache Pain 2008;9:19-27.ArticlePubMedPMCPDF
- 26. Onderwater GLJ, van Oosterhout WPJ, Schoonman GG, Ferrari MD, Terwindt GM. Alcoholic beverages as trigger factor and the effect on alcohol consumption behavior in patients with migraine. Eur J Neurol 2019;26:588-595.ArticlePubMedPDF
- 27. Panconesi A, Franchini M, Bartolozzi ML, Mugnai S, Guidi L. Alcoholic drinks as triggers in primary headaches. Pain Med 2013;14:1254-1259.ArticlePubMed
- 28. Slutske WS, Piasecki TM, Nathanson L, Statham DJ, Martin NG. Genetic influences on alcohol-related hangover. Addiction 2014;109:2027-2034.ArticlePubMedPMC
- 29. Yokoyama M, Suzuki N, Yokoyama T, et al. Interactions between migraine and tension-type headache and alcohol drinking, alcohol flushing, and hangover in Japanese. J Headache Pain 2012;13:137-145.ArticlePubMedPMCPDF
- 30. Wall TL, Shea SH, Luczak SE, Cook TA, Carr LG. Genetic associations of alcohol dehydrogenase with alcohol use disorders and endophenotypes in white college students. J Abnorm Psychol 2005;114:456-465.ArticlePubMed
- 31. Krymchantowski AV, da Cunha Jevoux C. Wine and headache. Headache 2014;54:967-975.ArticlePubMed
- 32. Landini L, Souza Monteiro de Araujo D, Chieca M, et al. Acetaldehyde via CGRP receptor and TRPA1 in Schwann cells mediates ethanol-evoked periorbital mechanical allodynia in mice: relevance for migraine. J Biomed Sci 2023;30:28.ArticlePubMedPMCPDF
- 33. Husain K, Mejia J, Lalla J, Kazim S. Dose response of alcohol-induced changes in BP, nitric oxide and antioxidants in rat plasma. Pharmacol Res 2005;51:337-343.ArticlePubMed
- 34. Mathew RJ, Wilson WH. Regional cerebral blood flow changes associated with ethanol intoxication. Stroke 1986;17:1156-1159.ArticlePubMed
- 35. Panconesi A. Alcohol-induced headaches: evidence for a central mechanism? J Neurosci Rural Pract 2016;7:269-275.ArticlePubMedPMC
- 36. Paolucci M, Altamura C, Vernieri F. The role of endothelial dysfunction in the pathophysiology and cerebrovascular effects of migraine: a narrative review. J Clin Neurol 2021;17:164-175.ArticlePubMedPMCPDF
- 37. Iyengar S, Johnson KW, Ossipov MH, Aurora SK. CGRP and the trigeminal system in migraine. Headache 2019;59:659-681.ArticlePubMedPMCPDF
- 38. Moon HS, Chung PW, Kim BK. New targeted drugs for acute treatment of migraine. Korean J Headache 2023;24:56-65.
- 39. Lu S, Zhang Y, Yang Y, et al. Hangover headache and its behavioral changes in rats. Iran J Basic Med Sci 2023;26:326-334.ArticlePubMedPMC
- 40. Cheng Y, Liu X, Ma X, Garcia R, Belfield K, Haorah J. Alcohol promotes waste clearance in the CNS via brain vascular reactivity. Free Radic Biol Med 2019;143:115-126.ArticlePubMed
- 41. Olesen J. Provocation of attacks to discover migraine signaling mechanisms and new drug targets: early history and future perspectives - a narrative review. J Headache Pain 2024;25:105.ArticlePubMedPMCPDF
- 42. Kim DJ, Kim W, Yoon SJ, et al. Effects of alcohol hangover on cytokine production in healthy subjects. Alcohol 2003;31:167-170.ArticlePubMed
- 43. Ha WS, Chu MK. Altered immunity in migraine: a comprehensive scoping review. J Headache Pain 2024;25:95.ArticlePubMedPMCPDF
- 44. Gao XM, Dong WH, Xia CL, et al. Centranthera grandiflore alleviates alcohol-induced oxidative stress and cell apoptosis. Chin J Nat Med 2022;20:572-579.ArticlePubMed
- 45. Wu D, Zhai Q, Shi X. Alcohol-induced oxidative stress and cell responses. J Gastroenterol Hepatol 2006;21 Suppl 3:S26-S29.ArticlePubMed
- 46. Jiménez-Jiménez FJ, Alonso-Navarro H, García-Martín E, Espada-Rubio S, Agúndez JAG. Oxidative stress and migraine. Mol Neurobiol 2024;61:8344-8360.ArticlePubMedPDF
- 47. Panula P. Histamine, histamine H3 receptor, and alcohol use disorder. Br J Pharmacol 2020;177:634-641.ArticlePubMedPMCPDF
- 48. Rossetti I, Zambusi L, Maccioni P, et al. Predisposition to alcohol drinking and alcohol consumption alter expression of calcitonin gene-related peptide, neuropeptide Y, and microglia in bed nucleus of stria terminalis in a subnucleus-specific manner. Front Cell Neurosci 2019;13:158.ArticlePubMedPMC
- 49. Gardiner C, Weakley J, Burke LM, et al. The effect of alcohol on subsequent sleep in healthy adults: a systematic review and meta-analysis. Sleep Med Rev 2025;80:102030.ArticlePubMed
- 50. Roberts E, Smith R, Hotopf M, Drummond C. The efficacy and tolerability of pharmacologically active interventions for alcohol-induced hangover symptomatology: a systematic review of the evidence from randomised placebo-controlled trials. Addiction 2022;117:2157-2167.ArticlePubMedPDF
- 51. Mammen RR, Natinga Mulakal J, Mohanan R, Maliakel B, Illathu Madhavamenon K. Clove bud polyphenols alleviate alterations in inflammation and oxidative stress markers associated with binge drinking: a randomized double-blinded placebo-controlled crossover study. J Med Food 2018;21:1188-1196.ArticlePubMed
- 52. Kaivola S, Parantainen J, Osterman T, Timonen H. Hangover headache and prostaglandins: prophylactic treatment with tolfenamic acid. Cephalalgia 1983;3:31-36.ArticlePubMedPDF
- 53. Khan MA, Jensen K, Krogh HJ. Alcohol-induced hangover. A double-blind comparison of pyritinol and placebo in preventing hangover symptoms. Q J Stud Alcohol 1973;34:1195-1201.ArticlePubMed
- 54. Kim H, Kim YJ, Jeong HY, et al. A standardized extract of the fruit of Hovenia dulcis alleviated alcohol-induced hangover in healthy subjects with heterozygous ALDH2: a randomized, controlled, crossover trial. J Ethnopharmacol 2017;209:167-174.ArticlePubMed
- 55. Eriksson CJP, Metsälä M, Möykkynen T, et al. L-cysteine containing vitamin supplement which prevents or alleviates alcohol-related hangover symptoms: nausea, headache, stress and anxiety. Alcohol Alcohol 2020;55:660-666.ArticlePubMedPDF
- 56. Lee MH, Kwak JH, Jeon G, et al. Red ginseng relieves the effects of alcohol consumption and hangover symptoms in healthy men: a randomized crossover study. Food Funct 2014;5:528-534.ArticlePubMed
- 57. Lee HS, Isse T, Kawamoto T, Baik HW, Park JY, Yang M. Effect of Korean pear (Pyruspyrifolia cv. Shingo) juice on hangover severity following alcohol consumption. Food Chem Toxicol 2013;58:101-106.ArticlePubMed
- 58. Jang YL, Park MK. Advanced clinical symptoms of the antihangover compound HK-GCM-H01 in healthy Koreans. Transl Clin Pharmacol 2024;32:137-149.ArticlePubMedPMCPDF
- 59. Verster JC, Dahl TA, Scholey A, Iversen JM. The effects of SJP-001 on alcohol hangover severity: a pilot study. J Clin Med 2020;9:932.ArticlePubMedPMC
- 60. Bogin RM, Nostrant TT, Young MJ. Propranolol for the treatment of the alcoholic hangover. Am J Drug Alcohol Abuse 1987;13:175-180.ArticlePubMed
- 61. Verster JC, van de Loo AJAE, Benson S, Scholey A, Stock AK. The assessment of overall hangover severity. J Clin Med 2020;9:786.ArticlePubMedPMC
- 62. Zhang H, Qi JZ, Zhang ZH. Comparative efficacy of different treatments for menstrual migraine: a systematic review and network meta-analysis. J Headache Pain 2023;24:81.ArticlePubMedPMCPDF
- 63. Lipton RB, Ailani J, Mullin K, et al. Situational prevention: pharmacotherapy during periods of increased risk for migraine attacks. Headache 2024;64:859-864.ArticlePubMed
- 64. Kim BS, Chung PW, Chung JM, et al. Evidence-based recommendations on pharmacologic treatment for migraine prevention: a clinical practice guideline from the Korean Headache Society. Headache Pain Res 2025;26:5-20.ArticlePDF
- 65. Bertz R, Bhardwaj R, Morris BA, Ashbrenner E, Coric V, Croop R. A placebo-controlled, randomized, single and multiple dose study to evaluate the safety, tolerability, and pharmacokinetics of rimegepant in healthy participants. Cephalalgia 2023;43:3331024231179131.ArticlePubMedPDF
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
- Related articles

Figure 1.
| A. Any headache fulfilling criterion C |
| B. Alcohol has been ingested |
| C. Evidence of causation demonstrated by all of the following: |
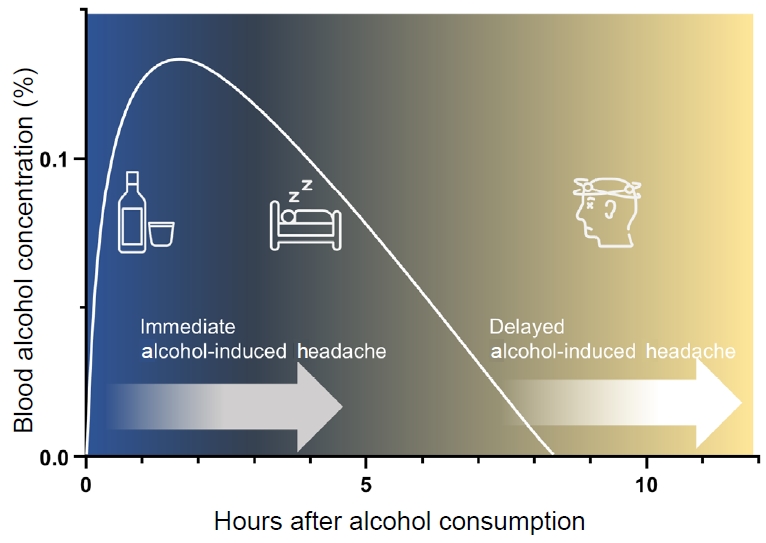
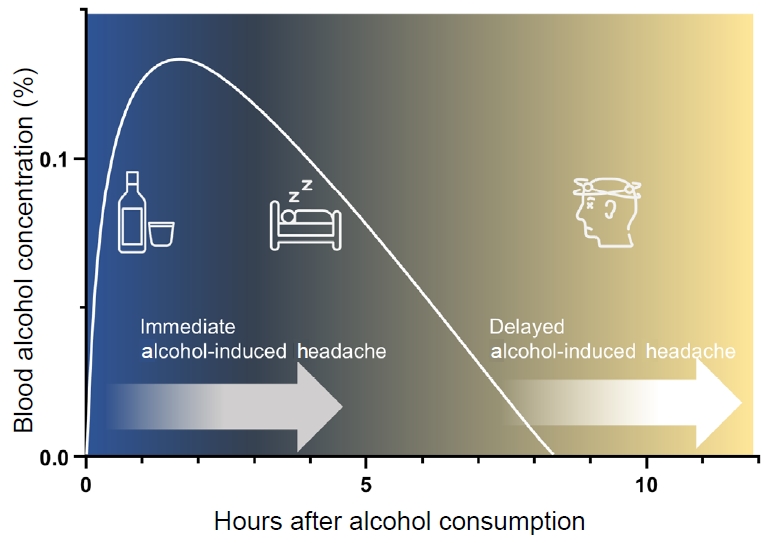
| 1. headache has developed within 3 hours of alcohol ingestion |
| 2. headache has resolved within 72 hours after alcohol ingestion has ceased |
| 3. headache has at least one of the following three characteristics: |
| a) bilateral |
| b) pulsating quality |
| c) aggravated by physical activity |
| D. Not better accounted for by another ICHD-3 diagnosis. |
| A. Any headache fulfilling criterion C |
| B. Alcohol has been ingested |
| C. Evidence of causation demonstrated by all of the following: |
| 1. headache has developed within 5–12 hours after ingestion of alcohol |
| 2. headache has resolved within 72 hours of onset |
| 3. headache has at least one of the following three characteristics: |
| a) bilateral |
| b) pulsating quality |
| c) aggravated by physical activity |
| D. Not better accounted for by another ICHD-3 diagnosis. |
| Domain | Alcohol-triggered migraine | Delayed alcohol-induced headache |
|---|---|---|
| Onset | Variable; often within hours | Within 5–12 hours of consumption |
| Duration | 4–72 hours | Mostly <10 hours |
| Location | Unilateral | Bilateral, frontal dominant |
| Quality | Pulsating | Pressing>pulsating |
| Aggravation by activity | ++ | ++ |
| Nausea/vomiting | ++ | ++ |
| Photophobia/phonophobia | ++ | + |
| Fatigue, dizziness, tremor | ± | ++ |
| Cranial autonomic symptoms (lacrimation, conjunctival injection, etc.) | - | + |
| Systemic autonomic symptoms (sweating, palpitation, etc.) | - | + |
ICHD, International Classification of Headache Disorders.
ICHD, International Classification of Headache Disorders.
Although both entities are classified as distinct entities within the International Classification of Headache Disorders, 3rd edition framework, this table is intended as a pragmatic tool for clinical differentiation rather than a nosological proposal.
Table 1.
Table 2.
Table 3.
TOP

